
Does Cannabis Help Treat Neuropathic Pain?
I discovered during my research that there remains a paucity of clinical data on cannabis for treating skin and many other disorders. However, the bandwagon of research clearly is the use of cannabis in treating numerous forms of pain, including a very special type called neuropathic pain. Here, there exists a wealth of information.
WHAT IS NEUROPATHIC PAIN?
From WebMD:
Neuropathic pain is a complex, chronic pain state that usually is accompanied by tissue injury. With neuropathic pain, the nerve fibers themselves may be damaged, dysfunctional, or injured. These damaged nerve fibers send incorrect signals to other pain centers. The impact of nerve fiber injury includes a change in nerve function both at the site of injury and areas around the injury.
One example of neuropathic pain is called phantom limb syndrome. This rare condition occurs when an arm or a leg has been removed because of illness or injury, but the brain still gets pain messages from the nerves that originally carried impulses from the missing limb. These nerves now misfire and cause pain.
Causes of Neuropathic Pain
Neuropathic pain often seems to have no obvious cause; but, some common causes of neuropathic pain include: Alcoholism, Amputation, Back, leg, and hip problems, Chemotherapy, Diabetes, Facial nerve problems, HIV infection or AIDS, Multiple sclerosis, Shingles, Spine surgery
Symptoms of Neuropathic Pain
Neuropathic pain symptoms may include: Shooting and burning pain, Tingling and numbness
I have considerable experience treating neuropathic pain starting at Rancho Los Amigos hospital in Duarte, CA. This was where many gang members ended up after a stabbing or other trauma. It’s where we preformed nerve blocks specially prescribed to help this agonizing condition. Years later, I’d treat patients using acupuncture and Chinese herbs as an effective adjunct to conventional approaches.
Some forms like RSD (see below) are crippling and lead to a high disability rate. Once you have a diagnosis of this condition you will begin treating it like a new career. It’s relentless, very painful, and unresponsive to modern medicine.
Reflex Sympathetic Dystrophy (RSD) leads to a shriveled, cold, painfully sensitive arm (if it occurs there). Over time the limb contracts, loses its hair, the skin becomes shiny and atrophic, it becomes cold, the nails thicken and brown, and of course there’s pain. The pain is unusual too. It’s often shock-like, or tingly, or painfully cold or even hot. The slightest thing like a breeze can be horrifyingly tender to the ultra-sensitive skin. The list goes on.
Sure we can get temporary relief using nerve blocks, opiates, and antidepressants but this is a condition that goes down fighting. They always come back for further therapies because there’s never much relief past about one week using invasive nerve blocks, and that’s the best we have.
If there were ever a reason to use medical marijuana this is the case. The drugs we often use have terrible side effects like dry mouth and excessive sedation. Of course chronic opiate use is still employed which leads to dependence. Yet opiates do not treat this type of pain very effectively.
ENTER CANNABIS
From the World Congress on Pain held in 2014:
Treating Neuropathic Pain with Cannabis: Pro and Con
Debate-style session at World Congress on Pain focuses on safety, efficacy of marijuana for neuropathic pain
A vote for efficacy
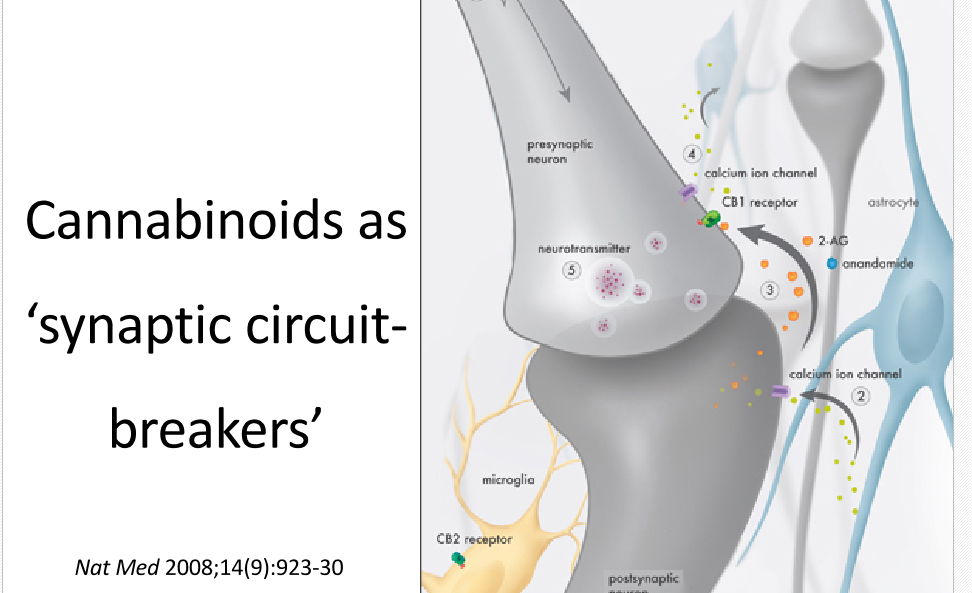
The scientific rationale for the use of cannabinoids in pain is clear, Ware explained: Throughout the nervous system, endogenous cannabinoids act as synaptic circuit breakers. These small lipid neuromodulators bind to specific receptors on presynaptic terminals, where they block the release of neurotransmitters. Because their receptors are widespread, cannabinoids, whether endogenous, plant-derived, or synthetic, regulate neurotransmission in many circuits, including in pain-producing pathways (for a complete overview of cannabinoids in pain, see Hohmann and Rice’s Chapter 38 in the Wall and Melzack’s Textbook of Pain, Sixth Edition, 2013). To the extent that neuropathic pain stems from abnormal neuronal activity, it makes sense that cannabinoid receptor (CB) agonists should be analgesic, and their effectiveness has been shown in many models of neuropathic pain in animals, using both natural and synthetic cannabinoids.[ref](http://www.painresearchforum.org/news/48905-treating-neuropathic-pain-cannabis-pro-and-con) 06/18/2015[/ref]
In the next installment I’ll go into much greater detail on the pros and cons of using this new, novel, pain reliever called cannabis.
***
Let’s continue our discussion of cannabis in the treatment of neuropathic pain with a spirited soliloquy from the World Congress on Pain.
Taking the pro side was Mark Ware, a pain clinician at McGill University, Montreal, Canada. Ware is the director of clinical research at the Alan Edwards Pain Management Unit at McGill and director of the nonprofit Canadian Consortium for the Investigation of Cannabinoids (CCIC). On the con side was Andrew S.C. Rice, Professor of Pain Research at Imperial College, London, UK. Rice, who is also a practicing pain clinician, has done research on cannabinoids and their use for pain.[ref](http://www.painresearchforum.org/news/48905-treating-neuropathic-pain-cannabis-pro-and-con) 06/19/2015[/ref]
Compelling evidence already exists in the literature which supports cannabis as an effective and safe medication in the treatment of the relentless pain of neuropathy. We even have a scientists dream: a model that can explain the mechanism of pain relief. For patients who are victims of some of the most dreadful, and agonizing conditions that humanity could ever endure, hope is here!
Once again, endocannabinoids are proving to be worthy allies capable of mentally hamstringing the most truculent drug company scientists. In other words, this humble herb has a syllabus of “cures” that Big Pharma can only look at in astonishment. And all of it is natural.
Dr Ware explained that the cannabinoids act as modulators, “circuit breakers,” on numerous nervous pathways. Within these pathways, CB receptors are located at many key sensory intersections as seen in his Power Point slide of a nerve terminal (below).
Once the nerve is stimulated by an action potential (normal nerve conduction) endocannabinoids such as anandamide flow retrograde up to the PRESYNAPTIC terminal (see top bold arrow) to dampen the forward flow of nervous information. This leads to less pain impulses being generated and perceived. This decrease is interpreted as pain relief.
This model also clearly explains how and why cannabinoids are capable of arresting seizures that are treatment resistant. They decrease the flow of information thus stopping the seizure.
With the ability of the cannabinoids to attenuate nerve impulses it makes perfect sense that these substances could be excellent pain relievers. And they are. We already have proof from dozens of studies. Here’s an example:
Proof of efficacy. Dr Ware quoted an article from his decidedly antagonistic, protagonist Dr Rice (Phillips et al., 2010), which supports the use of smoked cannabis as an efficacious medicine in the treatment of HIV-associated sensory neuropathy (a type of neuropathic pain).
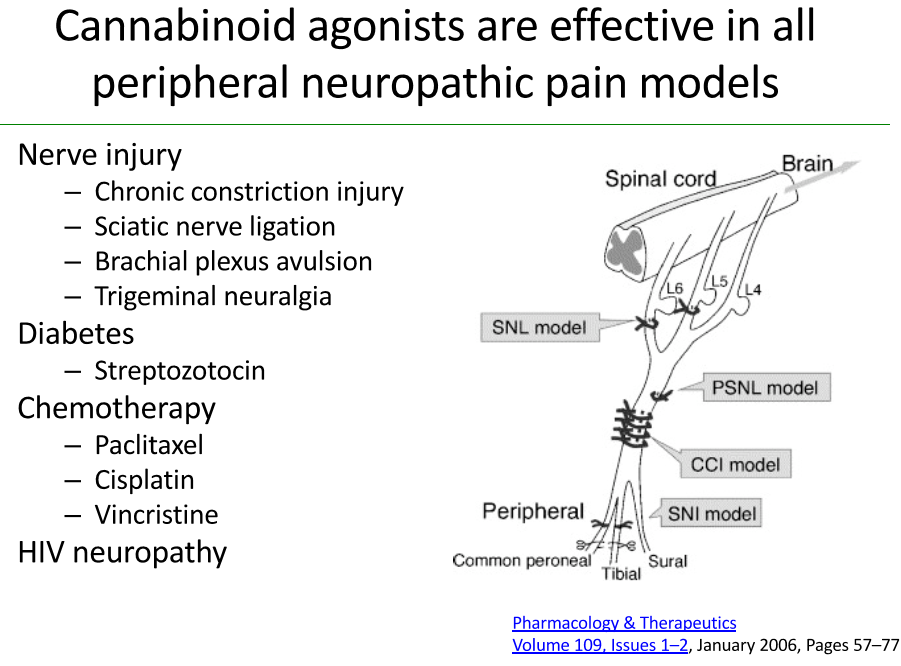
From Dr Ware’s Power Point presentation:

The below slide shows many other neuropathic conditions that respond positively to marijuana ingestion. Many of these are terribly painful conditions.
In clinical trials smoked cannabis is often times too difficult to quantify for scientific studies, Ware continued. That hurdle was somewhat overcome by the advent of vaporizers.
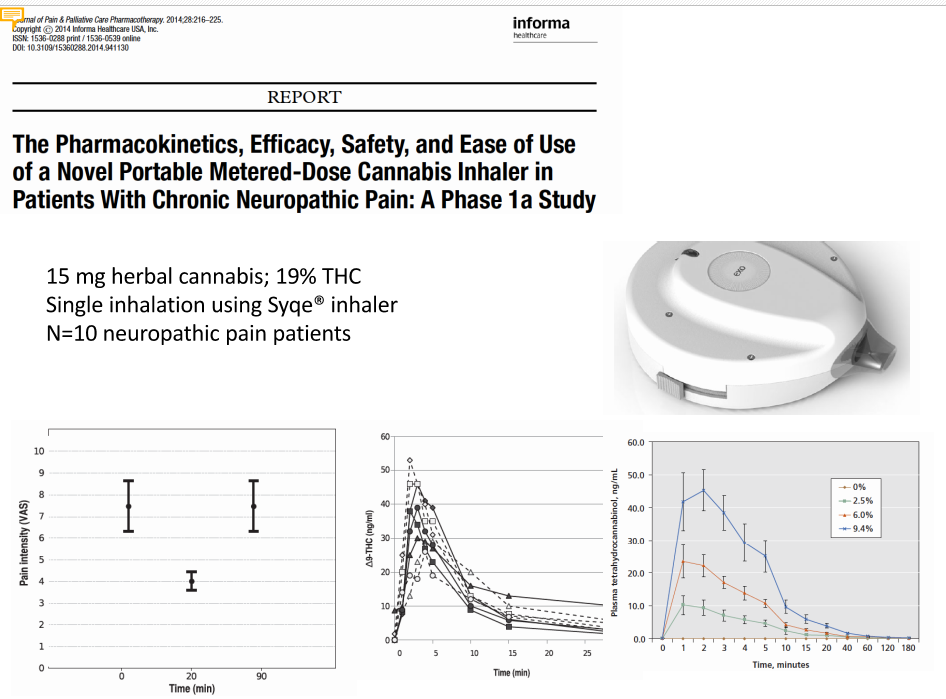
NEW HIGH-TECH DOSING
Perhaps even better that vaping is a new technology being developed which allows the user to inhale “granulated” cannabis much as you would use a rescue inhaler for asthma. This allows precise dosing that keeps blood levels below “recreational” so that the patient is pain free but not high. An example of the inhaler is shown below from Dr Ware’s Power Point presentation.
Dr Ware commented that many patients smoke marijuana because it relieves their pain, this is a patient driven industry, and drug companies are simply following up on promising leads.
Furthermore, the adverse effects of pot come mainly from those wishing to get stoned. Effects like impaired driving, psychosis, sedation, anxiety, tolerance, dependence, changes in cognitive function, orthostatic hypotension, and other effects.
This is not true with your average patient seeking relief from pain. They are not necessarily vying for a recreational stoning.
***
In the last segment from the World Congress on Pain, Dr Ware was featured as the supporter of medical cannabis. On the con side was Dr Rice, who concedes that animal data clearly support the use of cannabis for pain. However, studies involving humans are more equivocal.
Moreover, cannabis is not approved for treating neuropathic pain in any country. Rice does not endorse the use of pot for patients with neuropathic pain. He claims that there is accumulating evidence of long-term harms associated with cannabis use. “Is it safe?” Rice asked. “I don’t know.”
LONG TERM HARMS?
He goes on to quote several studies that show an increased risk for psychosis. A meta-analysis of seven studies demonstrated a three-fold increase in the risk for psychosis among users of marijuana (Semple et al., 2005).
This becomes an even greater concern, he reminds us, since the potency of cannabis has increased fourfold over the last 30 years (Volkow et al., 2014).
There is also some question of cognitive decline as some studies suggested that this occurs in those who start smoking in adolescence and continue into their late 30’s.
Rice then refers to the diet drug Rimonabant (an endocannabinoid antagonist). Sadly, its use led to higher rates of depression and suicide. It was removed from the market several years ago.
That shows the dangers of tinkering with the cannabinoid system in the brain, Rice said. It also highlights the critical need for long-term follow up in future clinical trials of cannabis or cannabinoids.[ref]IBID[/ref]
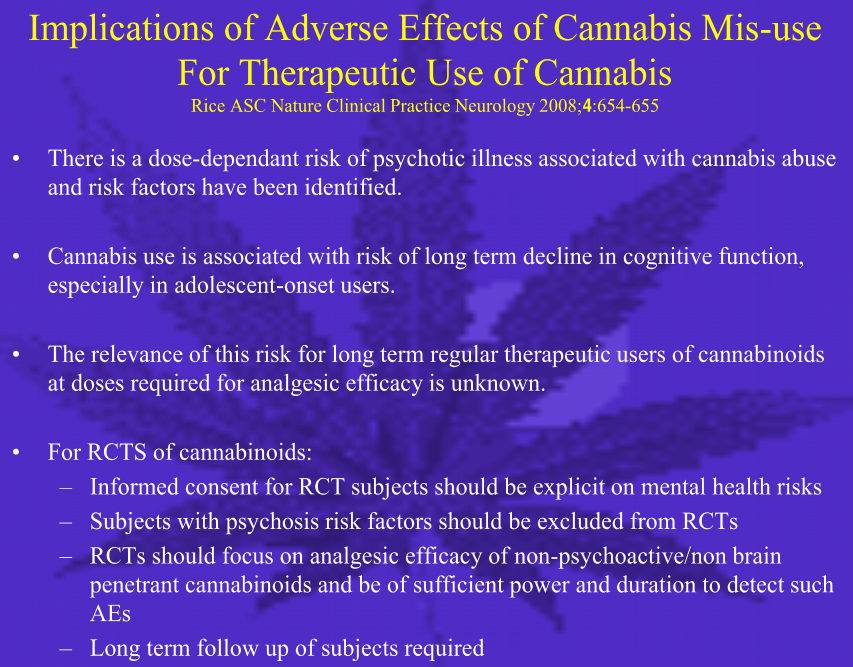
From the Power Point slide shown below from the World Congress on Pain. Dr Rice’s main concerns are the increased risk for psychosis and cognitive decline. His talking points are summarized in the Power Point slide that he presented (see below).
Stop for a moment and appreciate what neuropathic pain is all about; managing the pain will become your new career. That’s because many forms are excruciating and demand your attention at all times. While there is no effective treatment, you’ll still be taking many drugs in a wretched attempt to placate the anguish.
As Elvis Costello chirped in his bemused fashion: “I used to be disgusted, now I try to be amused.” That might be an appropriate response when we realize that patients are swimming in an ocean of polypharmacy. It’s become a risk factor for increased mortality. A study from Kaiser California showed that the average patient aged 60 is on over 30 medications! We could certainly use safer drugs if we had them.
NOT A VERY CONVINCING ARGUMENT DR RICE
Now can I get a volunteer please? Tell the poor soul ravaged by the scourge of neuropathic pain that you don’t approve of him using cannabis. Tell him no, even if it greatly helps his condition.
When asked why, you’ll tell him there’s a small risk of psychosis (in adolescents only), and after decades of using marijuana your memory or ability to juggle numbers may possibly diminish.
I find that argument amusing. This same doctor would have no problem prescribing, for example, a statin which can cause neurodegeneration and total global amnesia (see Dr Graveline’s book Lipitor Thief of Memory). But lord forbid, don’t prescribe a plant extract with a safety profile better than sugar.
This attitude is very common among community doctors and scientific researchers. It displays a bias toward drug company pharmaceuticals which only slows down our progress in cannabis research.
***
Most of the reluctance to use marijuana is due to a concern among physicians that there is insufficient data to support safety in long-term use of marijuana for neuropathic pain conditions. Those concerns were mostly in the orbit of increased risk for psychosis and cognitive decline.
However, we are not talking about treating kids. Only when kids start smoking pot at an early age is the risk for psychosis great and only to those genetically at risk. But teens and tweens are at greater risk for schizophrenia anyway, with or without using pot. Furthermore, some studies suggest only an association with pot smoking and psychosis not causation. Kids with emerging thought disorders need to avoid marijuana in all of its forms.
Meanwhile, epidemiologic evidence suggests that there is little risk for adults. We have an entire generation of Baby Boomers who love smoking pot. We have no evidence that they suffer from cognitive decline or are at increased risk for psychosis.
We are concerned with adult patients suffering severe and intractable pain which is resistant to conventional therapy. Here the cannabinoids could be a safe and efficacious treatment. From the World Congress on Pain:
Going forward, Rice said, researchers should aim at improving the therapeutic index of cannabinoids, including identifying non-psychoactive analogues and non-brain-penetrant analogues that can produce analgesia at sites outside of the central nervous system. In addition, he pointed to ongoing clinical trials with fatty acid amide hydrolase (FAAH) and monoacylglycerol (MAG) lipase inhibitors, which prevent breakdown of endogenous cannabinoids.[ref](http://www.painresearchforum.org/news/48905-treating-neuropathic-pain-cannabis-pro-and-con) 06/20/2015[/ref]
The above demonstrates laudable goals. I am in total agreement. Yet, these dream drugs are years away. It will take 5-10 years before we would see any of them commercially available.
Dr Ware (from the World Congress on Pain, see previous article) added that although there are very promising pharmaceutical approaches in the pipeline, these desperate patients need something NOW.
We have patients struggling now and need to figure out how to use this today.[ref]IBID[/ref]
Let’s take a closer look at some of the more compelling studies that offer sufficient proof for the average clinician to steer him or her in the direction of a cannabis recommendation.
LOW-DOSE VAPORIZED CANNABIS
In 2013 the Journal of Pain published a study that found the use of low dose vaporized cannabis an effective drug in the management of “treatment-resistant” neuropathic pain. The effects were just as good using low dose THC versus a higher dose which is curious. Based on this study a patient could achieve excellent pain relief without cognitive impairment. A plus for clinician and patient alike.
Vaporized cannabis, even at low doses, may present an effective option for patients with treatment-resistant neuropathic pain…
The analgesia obtained from a low dose of delta-9-tetrahydrocannabinol (1.29%) in patients, most of whom were experiencing neuropathic pain despite conventional treatments, is a clinically significant outcome. In general, the effect sizes on cognitive testing were consistent with this minimal dose. As a result, one might not anticipate a significant impact on daily functioning.[ref]J Pain. 2013 Feb;14(2):136-48.[/ref]
WONDERFUL NEWS FOR NEUROPATHIC PAIN PATIENTS
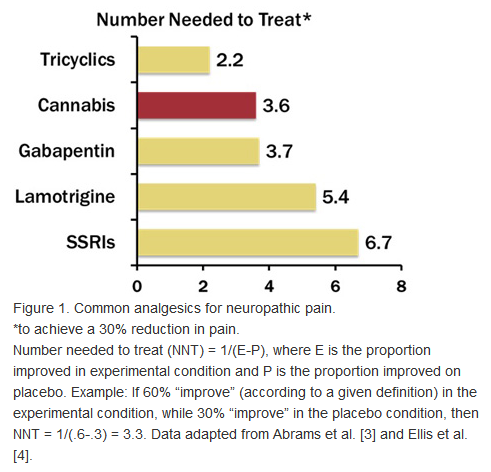
The AMA Journal of Ethics reported on recent research into the use of cannabis in treating painful peripheral neuropathy. This is a common type of neuropathic pain typically associated with diabetes but can be caused by HIV/AIDS, trauma, MS, adverse drug effects, and toxins.
One of the best drugs available in the treatment of neuropathy is called Elavil. Elavil is an old drug of the tricyclic antidepressant class. It has a “side effect” of relieving neuropathic pain. It’s also pretty debilitating even at low doses. It knocks you out while delivering a titanic “cotton mouth,” effect. It’s much stronger than the worst forms of dry mouth from smoking pot.
There’s a little gem hiding in this report. If you examine the figure below you’ll see that marijuana ranks nearly as powerful in the number needed to treat (NNTT) in order to relieve pain as the best we have, Elavil (under tricyclics).
Note also that the SSRI’s, and the drug company dog in search of a home, gabapentin and its wayward sister lamotrigine, look abysmal compared to cannabis. These pharmaceuticals are nearly worthless and have terrible side effects too.
***
CANNABIS RELIEVES ALLODYNIA
Below is another study out of many that clearly demonstrates the unique and potent ability of cannabis preparations to relieve agonizing neuropathic pain.
The University of Glasgow in the UK reports:
These findings demonstrate that, in a meaningful proportion of otherwise treatment- resistant patients, clinically important improvements in pain, sleep quality and SGIC (Subject Global Impression of Change) of the severity of their condition are obtained with THC/CBD spray,…THC/CBD spray was well tolerated and no new safety concerns were identified.[ref](http://www.unitedpatientsgroup.com/blog/2014/03/13/study-cannabis-effectively-treats-neuropathic-pain/) 06/20/2015[/ref]
This study focused on the relief of a novel form of pain called allodynia which is as maddening as it is crippling. Imagine a cool summer breeze causing your arm to feel as if it were on fire.
Allodynia is pain, generally on the skin, caused by something that wouldn’t normally cause pain. Many people with fibromyalgia report having this symptom. Examples of allodynia are pain caused by mild pressure from clothing, a light touch, gentle massage, or sheets rubbing against the skin.
Allodynia is believed to be a hypersensitive reaction that may result from central sensitization, which is associated with fibromyalgia.[ref](http://chronicfatigue.about.com/od/glossary/g/allodynia.htm) 06/20/2015[/ref]
This disorder is associated with many conditions not just fibromyalgia. As you might imagine, this ailment is terribly uncomfortable. Drugs simply do not help much. Usually by the time you receive some pain relief from pharmaceuticals you are pretty intoxicated and ready for bed. That, the ultra-dry mouth, the blurry vision and urinary retention, are usually enough to preclude one from taking these meds for any length of time.
OTHER TRIALS
The University of Glasgow provided a summary of recent studies supporting the role of cannabis in treating several types of neuropathic pain. We have already covered several of these from the list.
A 2011 study of the effects of smoked cannabis on HIV neuropathy found statistically significant improvement in pain, as well as mood and daily functioning.
According to a 2010 study, post-traumatic and postsurgical neuropathic pain can be effectively treated by smoking cannabis.
In 2011, researchers found that vaporized cannabis, even in low doses, helped with general and peripheral neuropathy in patients who didn’t find relief from traditional treatment.
A 2004 study found a clinically relevant analgesic effect from THC pills on neuropathy associated with multiple sclerosis.[ref](http://www.unitedpatientsgroup.com/blog/2014/03/13/study-cannabis-effectively-treats-neuropathic-pain/) 06/20/2015[/ref]
AND THE WINNER IS
The bottom line is that cannabis is a real winner.
It provides pain relief almost as good as the gold standard Elavil (or a similar TCA) without knocking you into next week. Its safety and side effect profile is unrivaled when compared to the shopping list of expensive, ineffective, and often toxic medications that are the mainstays of conventional medical therapy.
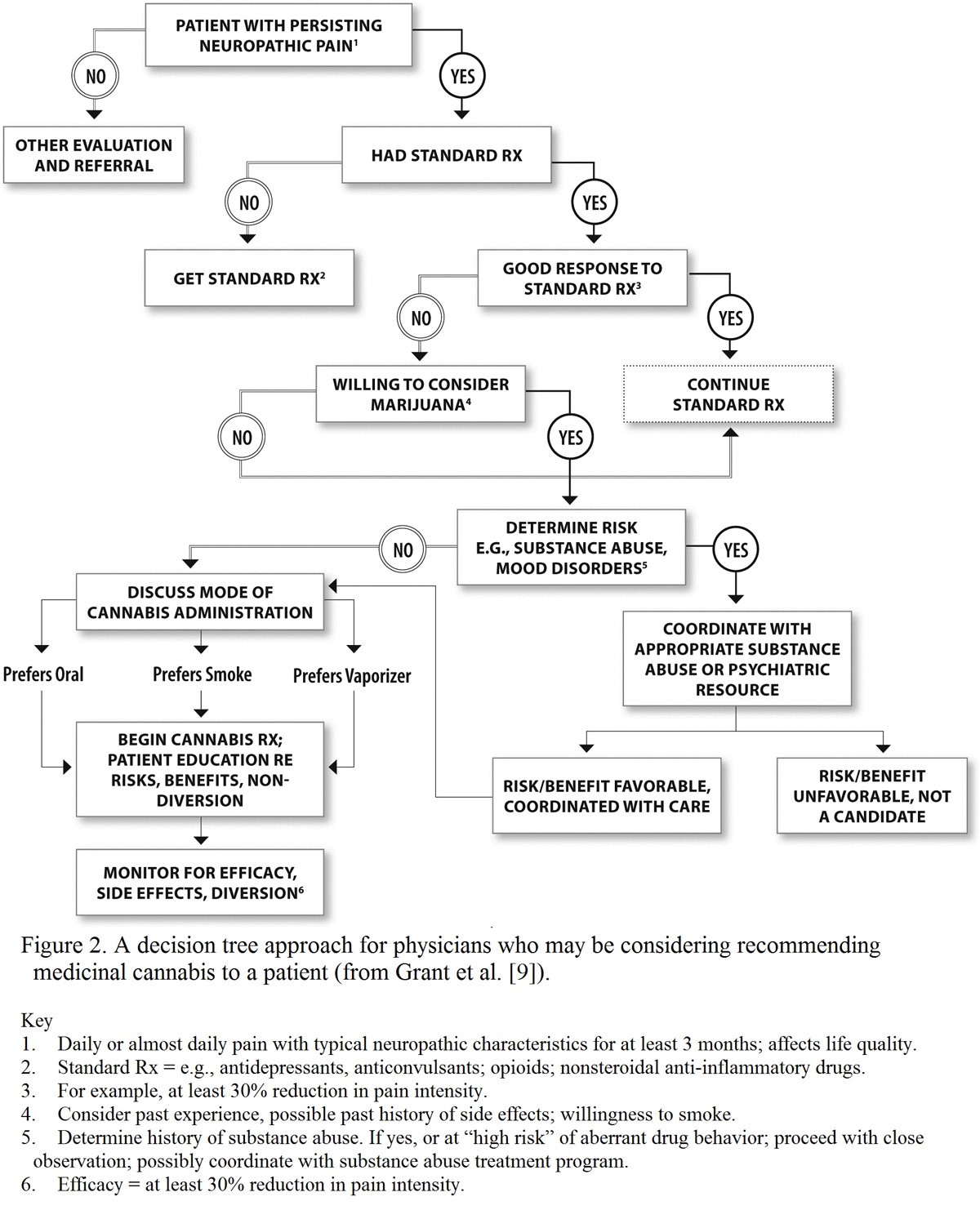
Below is a well-designed schematic approach for physician decision making in jurisdictions where medicinal cannabis is permitted.4 Note once again that this is cannabis WITH THC, not simple CBD oil.
Although smoking a marijuana cigarette is the most common form of self-medication, the authors of the studies cited prefer either an oral spray like Sativex®, or a vaporized product to ensure a safer, metered dose.
In summary, there is increasing evidence that cannabis may represent a useful alternative or adjunct in the management of painful peripheral neuropathy, a condition that can markedly affect life quality. Our society should be able to find ways to separate the medical benefits of making a treatment available to improve lives when indicated from broader social policy on recreational use, marijuana legalization, and unsubstantiated fears that medicinal cannabis will lead to widespread cannabis addiction.[ref](http://journalofethics.ama-assn.org/2013/05/oped1-1305.html) 06/20/2015[/ref]
Well said. Lastly, recall that the prevalence of diabetes is astronomical in the first world. Most of them will develop peripheral neuropathy. Let’s get the word out that these patients finally have a safe and effective drug to relieve their chronic pain.
I have neuropathy following spinal injuries. The symptoms of the are particularly bad at night time, especially when in bed. After unsuccessfully trying everything my GP could prescribe I turned to cannabis. The results have been absolutely spectacular. No more painful, restless nights and on the occasions when the pain is especially intense, I find the pain much easier to deal with. Would definitely recommend to anyone experiencing this soul destroying pain.
I too have neuropathic pain from a brain haemorrhage. How do I get cannabis oil in the UK though?
Is there any more recent news? I’m a desperate neuropathic pain sufferer as a result of arthritis in spine. When can we get something like sativex through the NHS?
I recomend you also take a look at mr Andrew Rice conflicts of Interests (slide nr 2 from the world congress). Not only is he paid by the industry, he is also a shareholder. So when he recomend we should wait for the industry before we start using cannabis as medicine; is it i the patient interest or is it his personal econmical interest speaking?.