
The Reasons Why Cannabis Kills Cancer
The Reasons Why Cannabis Kills Cancer
CANNABIS KILLS CANCER: SIMPLE BREW, PROFOUND CURE
Like me, you’ve probably been reading many of the anecdotal case reports of patients with deadly cancers curing themselves. They were using a simple alcohol extraction-essential oil of cannabis.
That’s it, an unpretentious kitchen-brewed elixir, no more drug company fabricated than spaghetti sauce. And far easier to make I’ll add.
Is there any real science behind the healing magic of this strange improbable material? Or is it just wishful thinking?
It’s much more than that. Even though we lack much needed human phase III clinical trials using cannabis we do have thousands of animal and tissue culture experiments that confirm weed’s healing powers.
THE ANTICANCER PROPERTIES OF THC
To date molecular biologists and clinicians have come up with a list of cancer fighting properties assigned to THC which we will discuss. CBD is much like THC in its anti-tumor properties. The other sixty plus cannabinoids may also play a role but what that is remains to be seen.
1. THC is anti-proliferative. Meaning that it inhibits cancer cells from reproducing. One of the hallmarks of cancer cells is that they keep replicating, they are immortal and unstoppable, that’s the problem. “THC inhibits protein synthesis so that tumors cannot grow.” (Dr. Donald Tashkin Pulmonary and Critical care UCSF)
2. An antiangiogenic effect. Here THC inhibits the ability of cancer cells to grow new blood vessels. Stop blood vessel formation and you prevent cancers from feeding and oxygenating thus encouraging their demise.
3. Anti-metastatic effect. THC prevents cancers from spreading from the main tumor into other parts of the body. Keeping a primary tumor from metastasizing is of paramount importance in reducing death rates in cancers. The mets are which generally kill the patient by disrupting organ function and starving the patient of vital nutrients.
4. THC has a powerful apoptotic effect. Meaning that THC induces cancer cells to commit suicide. This is a feature of normal cells but malignant cells have lost that ability so they live forever. This effect hastens the death of cancer cells while leaving normal cells untouched.
5. THC stimulates CB receptors on tumors to produce ceramide. Ceramide is a compound that enters cancer cells and inactivates the cell’s energy source the mitochondria. This leads to cell death.
The healing beauty of the cannabinoids hails from their “fat loving,” or lipophilic (in science-speak) property. This asset allows THC to enter the brain’s parenchyma (cells) without being stopped at the brain’s Check Point Charlie: the blood brain barrier (BBB).
Once inside the brain THC helps dissolve tumors.
Furthermore, this same property allows free access into all cells with CB receptors which is most of our trillions of cells.
Therefore, cancers cannot hide from cannabis.
A very lucky break for researchers was the discovery that cancer cells continue to make CB receptors on their cell walls. This allows the cannabinoids access to the cell, to program it to kill itself, and for all the healing magic to occur.
Ten years ago research by pioneer professor of molecular biology and biochemistry, Manuel Guzman (Spain) showed that rats with brain tumors injected with THC directly into their brains showed remarkable tumor regression and disappearance.
This directly led to hundreds of studies following up on the heels of this project.

Seven-Year-Old Treats Her Leukaemia in Nine Days
Seven-Year-Old Treats Her Leukaemia in Nine Days
THE INCREDIBLE STORY OF MYKAYLA COMSTOCK
Below is a case featuring the incredible story of a seven-year-old girl diagnosed with acute lymphoblastic leukaemia. Her cure in just nine days using cannabis oil demonstrates to the world the healing power of marijuana.
From the website BraveMykayla.com:
…If someone can accept giving their child dangerous pharmaceutical medications every single day; medicine that has many unwanted side effects and addictive properties, then why is it not just as acceptable to start with Cannabis before progressing on to the harsher medicine? Why should this medicine not be available to a child? I have yet to hear a reasonable answer as to why it shouldn’t.
Indeed, why not? We are all conditioned to accept cancer treatments as high-tech, painful, complicated and expensive. The above quote is actually one of the most honest and insightful comments that I have read regarding cannabis cures.
But treating cancer doesn’t have to be that way.
THE DOUBLE STANDARD
There exists a beastly double standard among mainstream oncologists and much of the medical community. On the one hand they use odious poisons called chemotherapeutics on their patients with the finesse of a Medieval savant. Far too many patients die prematurely; the mortality counts are legion. Many patients perish in pain, despair and loss of dignity.
In other words, oncologists routinely harm their patients either deliberately or through ignorance while watching them waste away from the demanding protocols of chemoradiation.
Yet, present these oncologists with an herb no more threatening than sweet basil and you would have thought their patients were asking to take suitcase bombs onto Capitol Hill.
NOW I TRY TO BE AMUSED
It’s entertaining when I read of some doctor’s mendacious concerns for the child’s safety and welfare when using cannabis. While still reciting the same fossilized script from 1942 when marijuana was removed from the US pharmacopoeia ending a thousand years of cannabis medicine; straight faced and sullen, they remind you that cannabis may harm your child.
Implying that marijuana is somehow more dangerous than the monstrously toxic drugs they intend on giving that same child.
Really?
They confidently voice their demurrals knowing full well that most of their “patients” will never recover from their treatment protocols; that most of them will be pushing daisies in six months to five years.
That’s actually laughable if it were not such a sad corruption of empathy and logic.
If these desperate patients are going to die anyway why not try something that, at the worst, will treat the dozens of adverse effects caused by chemoradiation while eliminating the half-dozen medications used to amend those symptoms.
At best it may even cure your patient.
Meanwhile, where does this hubris come from and why? What happened to compassionate care rather than staying cemented to arcane and perilous protocols that often lead to disfigurement and death?
It’s so strange it’s like living in Oz, err America.
Where’s the disconnect?
CUI PRODEST?
Since the attitude is so peculiar it must be driven by a deeper pathology. The disconnect is easily explained by examining who profits from this arrangement. Commercial medicine and Big Government profit handsomely from your cancer.
That’s why drug companies are currently heavily invested in chemotherapy. The greatest percentage of new drug applications are in chemo.
Or look at your city’s hospital campus which is more than likely building a new wing or cancer care center. Cancer is huge, it’s the new cash cow.
You’ll never get a reasonable answer to Mr. Comstock’s query until governments end their war on pot and allow both patients and doctors complete medical freedom.
In other words, it’s probably never going to change. Moreover, pot is cheap compared to the $100,000 price tag per chemo patient. To defend their position, drug companies will be lashing out against kitchen-made marijuana preparations as profits fall. Just wait you’ll see.
A preparation such as Rick Simpson Oil is seen as a dog that won’t hunt since it can’t be patented in that form. They prefer using expensive, patented medicines often times FDA approved through conflict-of-interest science. It’s also an enormous threat to them should momentum keep building and people demand marijuana oil over chemo.
Therefore, the biggest impediment toward change is the Commercial Sick Care System (CSCS) itself.
It is evolving into an enormous problem that could sink modern medicine. Over the last several decades this has led to entire fiefdoms (statins, SSRIs, chemo) commissioning ineffective drugs for patient care while charging usury rates.
Below is a quote from the former editor of one of the most prestigious medical journals in the world. She’s not alone.
It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgement of trusted physicians or authoritative medical guidelines [such as cancer protocols]. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine. – Dr, Marcia Angell, Physician, Author, Former Editor in Chief of the NEJM
It stings to read the above authoritative quote. When fighting for your life with end stage cancer you do not want to question whether your chemo protocol is scientifically based or not.
STOP ONCO-DEMOLITION, CANNABIS FIRST
It’s imperative that we “drive” this system in the opposite direction. That is, where we start out with the safest drugs first when treating cancers; that includes using unpatented materials like marijuana oil.
Far too often patients desperately sick from chemoradiation and out of options reach for the healing green–if not arrested while reaching for it.
But often times it’s too little too late at that point. So why the reluctance on the part of oncology to avoid cannabis until it can’t help?
It also puts pot to the task requiring that it behave supernaturally in its healing capacity at such a late stage of Onco-Demolition.
Offering cannabis to moribund, stage IV patients, some on the verge of death from pharmaceutical assault, is morally bankrupt in the sense that it should have been given much earlier. It’s like trying to resuscitate an autopsy at that point. Oncology should rethink the purpose of using marijuana and start proposing it at the beginning of the protocol or instead of it.
EXTRAORDINARY
Here’s the extraordinary part. In spite of those in stage IV disease, we still see marijuana do the most amazing things with some of these people. Below is an example of one such case.
It makes me wonder if Lazarus was given a snort of Rick Simpson Oil back in Ancient Palestine.
Demand change and demand that your child gets the right drug for the right condition. That means cannabis first. Let the oncologists treat their own children with chemoradiation if they still insist that weed is a toxic schedule I narcotic.
At least one family had the stomach to pursue the right course. Although it wasn’t easy, it paid off. They got to see their daughter beat a lethal blood cancer.
Kudos to the Comstock family!
CASE PROFILE: MYKAYLA COMSTOCK
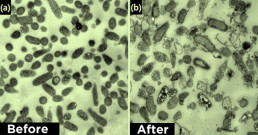
There is something enchanting about this little girl. Just hearing her happy voice is enough to moisten the eyes of the most hardened. The following case provides the reader with laboratory data of a dose-response induced remission using an extract of cannabis.
Mykayla Comstock was age 7 when diagnosed with acute lymphoblastic leukemia on July 14th, 2012. She fell ill in May and in July doctors discovered a large sized mass in her chest. From Mykayla’s father’s blog:
Mykayla was officially diagnosed with T-Cell Acute Lymphoblastic Leukemia on July 14, 2012, at only seven years old. T-cell ALL is a rare form of leukemia. It is an aggressive and fast-acting form of the childhood cancer. It is a cancer that is caused by the uncontrolled proliferation of Lymphoblasts into the body from the bone marrow. Lymphoblasts are immature cells which typically differentiate to form lymphocytes. Normally, lymphoblasts are found in the bone marrow only. These cells do not have the capability to die. Instead of going through a normal cellular life cycle, they remain, never succumbing to the natural programmed cell death. Instead, they are left to group together, forming a giant, liquid mucinous tumor that puts immense pressure on internal organs and wreaks havoc on a child’s immune system.[ref](http://www.bravemykayla.com/her-diagnosis.html) 11/17/2015[/ref]
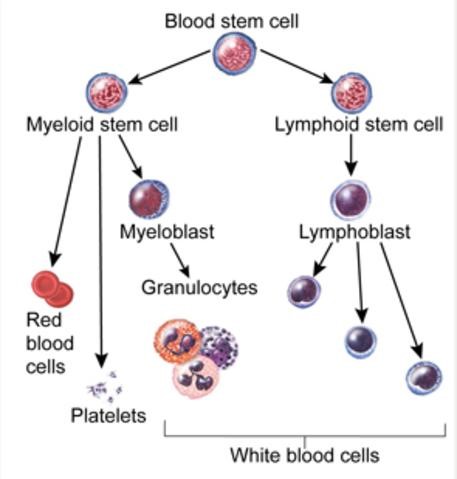
ALL IS A “BLAST.”
Below is a diagram of how immune cells are made. The “blasts” are the immature cells which proliferate in leukaemia.
In the US, the incidence of ALL is roughly 6000 new cases per year (as of 2009), or approximately 1 in 50,000. ALL accounts for approximately 70 percent of all childhood leukemia cases (ages 0 to 19 years), making it the most common type of childhood cancer. It has a peak incident rate of 2–5 years old…Based on the average $100,000 USD per patient, this gives the system 600 million dollars per year for just one type of cancer: ALL.
Mykayla’s oncologist started her on chemotherapy but she didn’t respond at all. An indicator of remission is when the blast count is under five percent.
The next approach might involve a stem cell (bone marrow) transplant. To treat brain lesions head radiation is considered. So little Mykayla, like the six thousand other ALL patients each year, was faced with the usual assaults from chemotherapy, surgical procedures, radiation and steroids.
This case appears similar to another case of ALL I reported on. In the previous case, (fourteen-year-old P.K. from Ontario, CA.), the patient died from chemo complications. Even though the Rick Simpson Oil (RSO, cannabis oil) put her ALL into remission it was started far too late. After numerous rounds of chemoradiation she was never able to recover.
This time the parents were able to prevent the decimation by getting on board with RSO earlier in the treatment. They could do this because Mykayla lives in a state with a medical marijuana program, and they were proactive.
POSITIVE CHANGE WITHIN ONE DAY
On day eleven (after ten days of chemo) they started marijuana. They followed the usual dosing schedule by having her consume a tiny grain-of-rice sized portion of Rick Simpson Oil (RSO). As expected she ended up considerably stoned. This is not always a bad side effect as so many doctors seem to think. Some patients actually enjoy it.
For the first time in weeks she had a smile on her face, was actually hungry and wanted to eat. Her father reports that during this time she kept telling him how happy she was while laughing at her illness.
But that’s nothing compared to what happened next.
REMISSION IN NINE DAYS
After only nine days of RSO she went into remission.
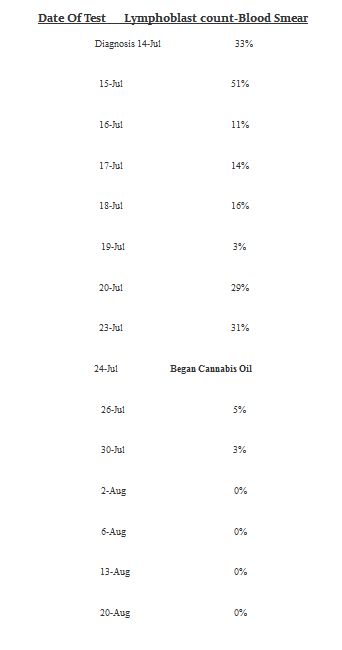
Mykayla’s chemo DID NOT affect her blast cell count (BCC). As you can clearly see (below) starting on July 14 with a BCC of 33% and ending on July 24 with a BCC of 31%.
Only when the new sheriff RSO rode into town did improvement occur.
Note that on July 23-26th there was an astonishing fall in her BCC from 31% to 5% after taking RSO. We do not have a BCC on the day the RSO was started. Let’s assume that it was 30% which is reasonable.
Therefore, in just two days it dropped from 30% down to 5% while consuming the emerald oil.
Dear oncologists everywhere, please note that in just nine days she was diagnosed in remission with ZERO blast cells.
Well done. Was the remission solely induced by RSO? There is no way to say for sure without follow up studies.
Below her father provides the hematology data regarding Mykayla’s ALL. Listed are the blast cell counts as percentages of total white blood cells. Zero, or close to it, indicates a remission.
Starting from July 14th 2012 to August 20th 2012 we have:
WE ARE CHILD PROTECTIVE SERVICES AND WE’RE HERE TO HELP
Those are the ten most dreadful words any parent could ever hear. Mykayla’s father was commenting on whether child protective services (CPS), festooned with shiny badges and clipboards, would be stealing across his front yard, commando style, to kidnap sweet little Mykayla away from her irresponsible parents bent on using dangerous, unproven marijuana oil treatments.
Which is always a possibility. If there had been a particularly misinformed official in CPS at the time this may have ended much differently.
Nevertheless, you should have absolute freedom in choosing how your own family will be medically treated especially now with the scientific upheaval in clinical drug research.
As you can see from the above quote by Marcia Angell MD, one of my heroes, the system is rigged and has been for decades. It’s based on junk science. So curing cancer with chemoradiation may be an ignis fatuus.
NOVEL CANNA-RESPONSE
Mykayla had an additional surprising and novel response to cannabis which should make it the leading drug for treating chemotherapy induced side effects independent of its tumor shrinking properties.
Compare the statement below (from her father) with the usual way people feel after chemotherapy.
As if her dramatic remission wasn’t amazing enough, Erin and I have observed a wide variety of benefits from Cannabis during Mykayla’s treatment. Cannabis has relieved nearly all of the horrid side-effects that we are warned about with each individual chemotherapy drug…Mykayla has needed the pharmaceutical anti-nausea medicine, Zofran, only a handful of times. She rarely, if ever, complains of pain anywhere; she hasn’t experienced the chemo-associated neuropathy (foot-drop)…when given Vincristine.
Another testament to the power of Cannabis is that Mykayla has currently experienced only one infection…. Cannabis is a powerful anti-biotic, anti-viral, and anti-fungal agent….
…Her spirits are always high, and she is always energetic. She continues to be creative and inquisitive despite the rigors of her treatment. Her mother and I attribute the majority of this to Cannabinoid Therapy.
AND YOU THOUGHT POT WAS GOING MAINSTREAM?
Regrettably, most hospitals and most doctors, even the best ones, can actually morph into a survival threat. In Gary Null’s publication entitled Death by Medicine, he explains how adverse drug reactions, hospital, and physician error are the number one cause of death in America.
Yet, what keeps these methods alive are that they maintain political correctness. You see the doctor reaching for patented medicines that are drug company compliant and consistent with the System’s business model, even if these drugs are ineffective.
Mykayla’s father commented on how tough they had it when deciding to employ a politically charged (read: non-patented, lifesaving) treatment option.
Based on the (below) remarks it appears as if there was some serious hostility from one oncologist. Her comments (in bold type) contain a little gem of wisdom that I’m sure she was not aware of.
Oncologists who treat Mykayla and other doctors and nurses have not volunteered their opinions. Our first oncologist constantly disagreed with us and eventually tried to forcibly refer us to another hospital, the reason being that she felt little Mykayla jeopardized the entire hospital including staff and patients….The few testimonies we have coaxed out of them are always fantastic. They have commented on how well her liver holds up during the hepato-toxic treatments they prescribe her. They see how smart and sharp she is through the neuro-toxic drugs regimens. They comment on how astonishing it is that she maintains her weight, never losing any for more than a day or two at a time. We know they know.
Mykayla proved to them that there is a better way. Here’s the gem: the oncologist warned that little Mykayla’s activities would jeopardize the entire system. She inadvertently implied that Mykayla’s novel and successful response using cannabis oil was far superior to their usual routines. Should anyone notice how superior RSO was it would jeopardize the entire hospital, staff and doctors who are forced into using dangerous and ineffective protocols.
Imagine a ward full of morose, vomiting children and little Mykayla sitting there all alone comfortably smiling, laughing and feeling high. Every caregiver on the floor would have noticed it.
Yes, that could unravel the con and clearly jeopardize the System. Let’s hope so.
MARIJUANA, THE ANTIDOTE TO CHEMO AND ALL
Conversely, in the same (above) quote, we see many hospital personnel did take notice. They were astonished at how well Mykayla swam through all of the drug-induced horror stories as if they were so much tripe.
But no one is coming out and saying the obvious-why?
Like the woolly mammoth eating TV dinners in your living room, nobody will acknowledge the simple fact that marijuana appears to be driving the entire syllabus of positive outcomes seen here.
A schedule I drug-of-abuse is really the cause of this wonderful outcome, including slating her leukaemia into remission.
Regrettably, to simply acknowledge the truth is not yet possible for physicians and care givers. Except for a small, vocal, fearless group who have the clinical knowledge, courage, and brains to recognize pot for what it is.
Marijuana may be the most valuable plant in the world.
There I said it.
We know that they see the difference. They see her giggle, run, dance, jump, and play, be hungry and want to experience life. Some nurses who have worked those wards for 15+ years have commented on how they have never before seen a child undergo so many poisonous treatments and handle it so well. They know she doesn’t have to take the seven prescription medications that she is offered for side-effect mitigation. Some medicines we have never used; they sit unopened in our cupboards just in case. Simply put, Cannabis has been a miracle for Mykayla; no one can argue this anymore, there is nothing left to debate. —
In 2015 Mykayla is reportedly doing great. She is still in remission, and is back doing what any kid her age is doing-enjoying her precious LIFE thanks to cannabis.
If your state does not have a medical marijuana program demand it from your congressman and state senators.

Man Treats Stage 4 Pancreatic Cancer Using Cannabis Oil
Man Treats Stage 4 Pancreatic Cancer Using Cannabis Oil
Hang on to your seats folks this one is impressive. Taken from YouTube (YT) I have included everything that’s relevant medically. However, as is common with YT, some data are missing such as Mr Rose’s age and some other points.
In 2013, Wallace Rose was examined by a doctor for complaints of stomach pain. A CT scan showed a pancreatic tumor. At the time it was small and surgical removal was considered a cure. Like 43 million other Americans he didn’t have insurance to cover the costs. His surgeon demanded a fee of ten thousand dollars and the OR charge was for six thousand. And it had to be cash up front!
After they had a fund raiser which took about six weeks he finally was operated on only to find that in the short period of approximately six weeks the tumor had geometrically expanded and metastasized.
It was now stage IV and incurable. It had spread to the liver, kidneys, and stomach in just six weeks. The surgeon closed the abdomen without being able to do anything for him.
It was December 18th that he received the worst news of his life: go home to die which will happen in about one month. Chemo was offered as a way to prolong his life by six to eight months but it would not cure him.
There was no cure.
With pancreatic cancer which is exceptionally aggressive, doctors can follow tumor markers as an indirect way of judging the extent of tumor involvement. It’s called CA 19-9 (see below left side under lab).
What is the CA 19-9 Radioimmunoassay (RIA) test? What does the CA 19-9 test measure?
The CA 19-9 Radioimmunoassay (RIA) is a simple blood test that measures the level of tumor-associated antigens found in the blood. Antigens are substances that cause the immune system to make a specific immune response. CA 19-9 antigens are foreign substances released by pancreatic tumor cells.
The normal range of CA 19-9 in the blood of a healthy individual is 0-37 U/ml (Units per milliliter).[ref](https://www.pancan.org/section-facing-pancreatic-cancer/learn-about-pan-cancer/diagnosis/ca19-9/) 11/17/2015[/ref]
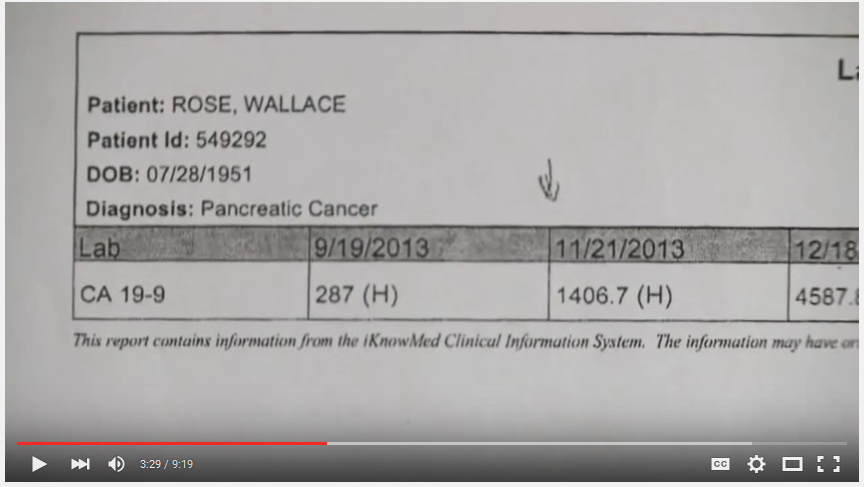
Above left column under lab shows the CA 19-9 and the patient’s name so we know it’s him.
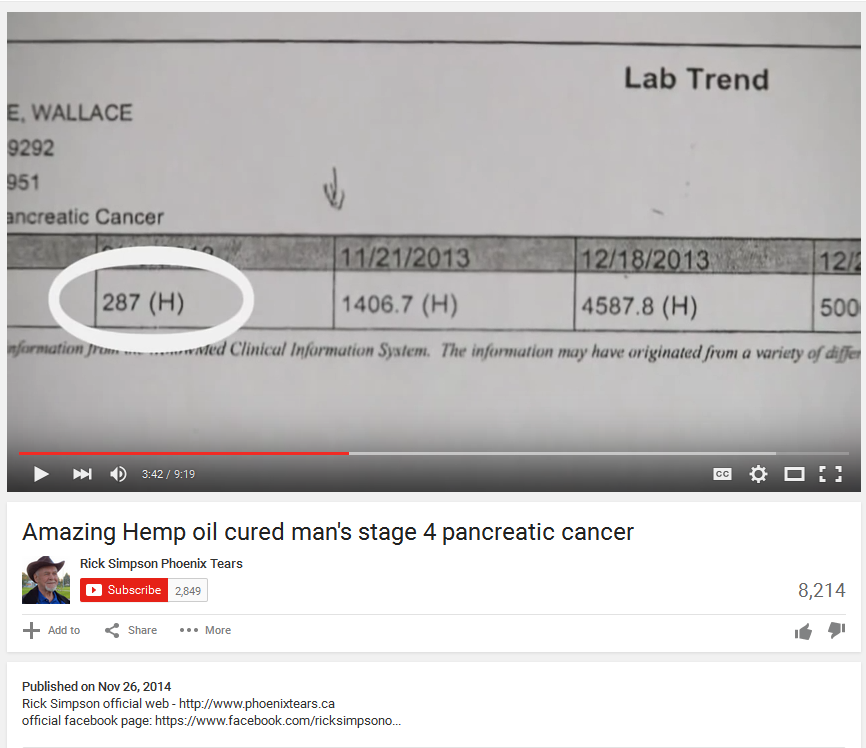
The first result from September came back at 287 (above) which was high but not terrible. The normal is under 37. Look now at the November value which was 1,406.7, an increase of 500% in two months! One wonders that if the surgeon had been less interested in money and more in doing what doctors are supposed to do, would he have been cured with the simple removal of a very small primary tumor?
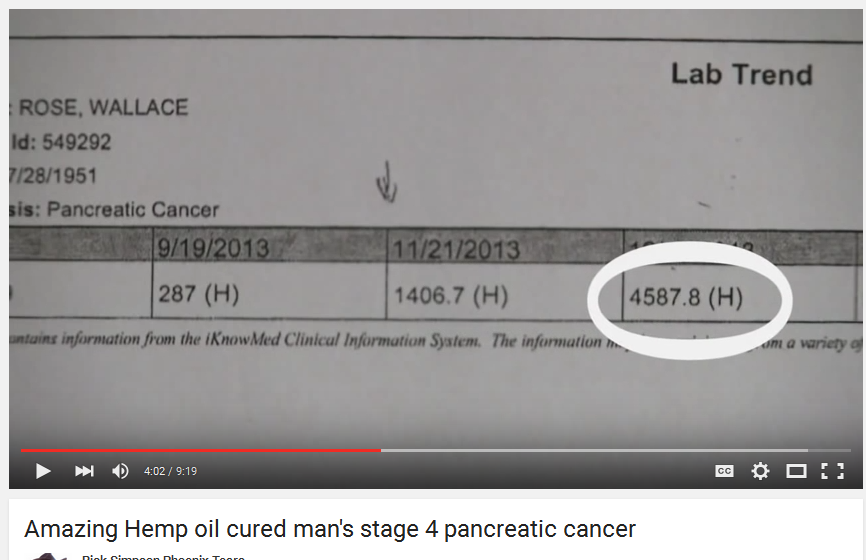
The next value really demonstrates the deadly kinetics of pancreatic cancer. Wallace went from 1400 in November to 4,587 by Dec 18 just shy of a month.
SATURATION POINT
The next image shows Wallace had reached a saturation point, that malignant cells were now everywhere in his body. This is a terminal event.
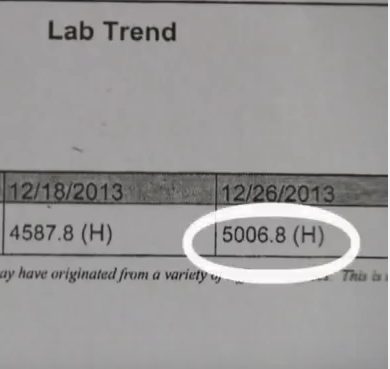
Based on the depressing news Mr Rose decided to invite all of his relatives for one last fling before he leaves planet Earth for good. That included inviting his enlightened relatives in Colorado who left him with a stocking stuffer containing 15 amps of Rick Simpson Oil (RSO)!
BEST MOVE EVER MADE
Out of desperation and convinced that RSO was simply a foolish attempt to promote marijuana by a couple pot heads, he started taking it after he got his license for its use from Dr Kathy Smith. With one month to live he averaged 2-3 grams of RSO per day. Note: the dosing Wallace used is up to three times more (three grams) than what most people take no matter how bad off they are.
But in this case it was incredibly intuitive and I believe the higher dose saved his life.
By Wallace’s own account he started the last few days of December through January, Feb, and March. Note also that he was taking two chemo drugs with the RSO: Abraxane and Gemzar. His doctor admitted that both of these drugs will not cure him. That they would only extend his life by 6-8 months. What we see here is a massive decrease in CA 19-9, going from 5,000 to 312 in about one month. It appears that he is going into remission.
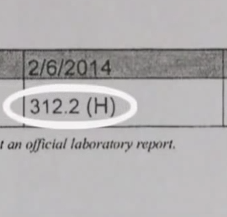
With uninterrupted dosing of RSO at 2-3 grams per day (plus chemo) we see further evidence of a remission (see below).
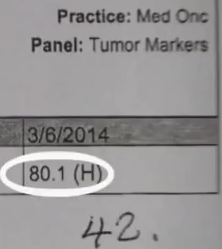
In one short month his value was now 80 and in free fall. The hand written number of 42 was his last value that I could find which was essentially normal. Stage IV pancreatic cancer is 100 percent fatal yet Wallace beat the odds with cannabis.
Mr Rose commented that he will be taking RSO for the rest of his life. He’ll probably outlive us all. This case provides further evidence of the astonishing properties of cannabis.
The Incredible Story of the Woman Who Shrunk her Tumours using Cannabis Oil
The Incredible Story of the Woman Who Shrunk her Tumours using Cannabis Oil
Whenever I find a great anecdotal report on a cannabis cancer cure (CCC) I like to inform people of its existence provided there is a threshold of proof that comes with the presentation. Dear reader, pass the word to all of those lucky patients around the world who have cured themselves of end stage cancers using cannabis to please provide MRI or CT evidence with their cases. If there is valuable blood work (such as a blast cell count with leukemia, or tumor markers) add that as well.
The best reason I can think of is to “turn” a recalcitrant doubting doctor, senator, congressman into one who becomes intrigued. There’s no way that will happen if you simply tell your story without any proof whatsoever. If you can get your doctor to vouch for it all the better.
After all, the tidal wave of cannabis legalization started only because it proved to have valuable medical uses. At this point in our history of cannabis change it’s important to ascertain if the “cure” indeed happened because of cannabis oil. That is, to rule out any fraud that may be occurring. That’s my job and I cannot do it with a simple testimony. The best cases are the ones that a physician helped write up complete with lab reports and imaging studies.
They are also the rarest. So far I have one such case that I have already published. I think many physicians are reluctant to publicly do or say anything that may alienate their status if they were to jump aboard the weed wagon and yell from the highest peaks that pot cures cancer. They are not going to publish or put themselves in the spotlight until this whole movement goes mainstream. I can’t really blame them either.
Now if cannabis does indeed cure some forms of cancer then we need to know which ones respond and how well they respond to it. That requires more detailed case reports and lots of clinical studies. It may turn out that some cancers like glioblastoma and breast cancer may be particularly sensitive to cannabinoids whereas other cancers may only respond partially.
Of course, ultimately knowing WHY the tumor responded is of the utmost importance. But that comes only from decades of research which grows daily.
We also need to know the dosing schedule: how much, how often? There are many product unknowns such as which types of cannabis are best, if any, at treating cancers. What is the most effective potency? In other words, is it really important to have very high potency THC or not? How much CBD should be in the mix? What about the other sixty-five or so cannabinoids? Also of concern is whether or not raw, unheated, cannabis has a role. If so what is it?
So far it looks like a gram per day of (the heated non-acidic form) RSO or cannabis oil is evolving to be the standard dose but maybe that needs to change. I have seen a handful of cases that only worked when the dosage was bumped up by two to three hundred percent: two to three grams per day. Sadly, we are far from knowing many of the basic facts about cannabis oil and treating cancer. But what we know so far is encouraging.
AN EMERGENCY
Moreover, cancers are off the charts so it’s becoming an emergency. At the rate that cancers are manifesting in a few more decades everyone will develop some form of cancer. The world is becoming more and more toxic and one of the results of that is cancer. Both people and pets are feeling this novel plague.
This is an important point because you may need to make a decision on whether you go conventional with “cut, poison, burn,” or go outside the box with raw cannabis juicing, hash oil or Rick Simpson Oil after you are diagnosed with a cancer.
In my book on preventive medicine I have a chapter on cancer prevention. Written as a guide to keep cancer out of your life it’s principles need to be followed. A new addition will be added that includes cannabis juicing and using the decarboxylated form as a way to keep cancer from forming on a cellular level. An ounce of prevention right? What would that dose be pray tell? Maybe it’s a gram of prevention or more per day.
I wish I had the time and resources to interview every northern California care giver and come up with a list of suggestions.
We need something yesterday because cancer is the new “it” girl and she’s not the one you’d like to marry.
Yes, the prevalence (the number of new cancer cases in a given population), is alarming; rising nearly geometrically from an obscure disease to the third leading killer in less than 100 years.
If you were to ask any gastroenterologist 40 years ago if a twenty-year-old kid could get colorectal cancer, he or she would most likely scoff and tell you that it’s rarer than steak tartar at that age group. Well not anymore. It’s becoming quite common now for adolescents and tweens to get the diagnosis that is normally reserved for the elderly. Rare types of cancer manifesting in the wrong age group indicates that things have taken a huge turn south. Like a canary in a coal mine it’s a warning that our world is far too toxic and that we are paying dearly for our Western ways of life.
Furthermore, the costs of treating cancer are ridiculously high. If that were not enough, consider the fact that most treatments are worthless. Chemotherapy helps about one in twenty while it sets a small percentage up for blood cancer decades later. That’s in addition to the tangle of chronic disorders patients must endure, should they survive, from the poisoning effect of chemoradiation.
CHEMOTHERAPY DOSING MAY BE BASED ON FRAUD
Even worse is the strange media headline (from a high-impact journal) that appeared two years ago indicating that most, if not all, basic animal research on chemotherapy drugs and cancers may need to be scrapped as essentially meaningless data. This had to do with fraud and conflict-of-interest science. If it’s true, it suggests that the oncology head literally does not know what the tail is doing. That the entire field of oncology is based on pseudoscience.
Well that’s no fun. It’s more than disconcerting to learn about this now as we spiral into a cancer pandemic.
The end result of having a cancer in the US (and perhaps the entire first world) is that typically you are poisoned with chemo drugs and radiation, your pocketbook is fleeced and you die bankrupt. Those countries that offer socialized medicine as in the UK at least leave you to die with your bank account intact. Not so in the good old USA.
Let’s look at the operose statistics. From Cannajournal.com:
I. 1 in 2 males will develop some form of cancer in their lifetimes. 1 of 4 of those will die from cancer. (source: cancer.org)
II. 1 in 3 females will develop some form of cancer in their lifetimes. 1 of 5 of those will die from cancer. (source: cancer.org)
III. In 2013 1,660,290 new cases of cancer were diagnosed in the US alone. In 2013 580,350 people died from various forms of cancer. (source: cancer.org)
IV. The cost to treat cancer oftentimes exceeds more than $100,000. (source: costprojections.cancer.gov)
V. Chemotherapy treatments are less than 3% successful (yes, a 97% failure rate) and are only effective in extending a patient’s life; it in no way cures cancer. (source: naturalnews.com) [Take this with a grain of salt-some cancers do respond to chemo for a cure but they are usually not the most common nor the deadliest. There’s only about 5 different cancers like Burkitt’s lymphoma that respond well.]
VI. Some current forms of cancer treatment involve the surgical removal of cancer sites, breasts, genitals, ect (sic). Oftentimes, cancers have been known to simply re-occur in new areas of an individual’s body years or even months after the surgery. (source: cancer.org)
VII. Society is losing the war on cancer. (source: kpbs news article)
VIII. I will add that we have LOST the war on cancer.
But the most menacing and far-reaching news is that the deadliest cancers are the most common and they are still the deadliest cancers. In other words, there are no cures for most cancers and chemo takes therapy in the wrong direction-it’s rather Medieval. These are not cures. That’s why when chemo helps they call it a remission not a cure. That way when it doesn’t work they have an out.
However, it is so lucrative that nobody in the system is ever going to suggest that it be changed even if it’s crazy to continue using these methods. Now granted some critics will contend that it’s not all doom and gloom and that the cure rates of some cancers have improved.
That may be true but, as I have said before, it’s too little too late. Statistically there is no change in the overall age-adjusted death rates for all cancers combined after 45 years of “the war on cancer.” Depressing to say the least.
Now that I have ruined your breakfast let me see if I can make your lunch bittersweet.
THE CASE REPORT

Let’s now examine the case study of 43 year old Cira Felina Bolla who was diagnosed with stage IV breast cancer. I’ll give you as much information as I can find but let me warn you that these cases are usually lacking something important.
Cira was originally diagnosed with Stage III Breast Cancer in early February 2013… She.. was able to do some initial tests and they have discovered it’s Stage IV. Then eventually diagnosed Triple Negative. She had to quit working the last week of February due to the pain in her back and from the tumor.
She started a Phase I Clinical Trial March 28th, 2013 to help destroy the tumor by targeting the mutated DNA and repairing it. Eventually Cira’s Tumor had shrank (sic) down to the size of a walnut…[ref](https://www.giveforward.com/fundraiser/4b34) 11/16/2015[/ref]
The first CT image taken from YouTube shows the initial scan which provides a snapshot of her baseline condition in March (2013). Note on the first image (below) the shadow in the top left quadrant between 9 and 10 o’clock (big arrow). That’s the initial breast tumor size which is very large as large as a big fist.
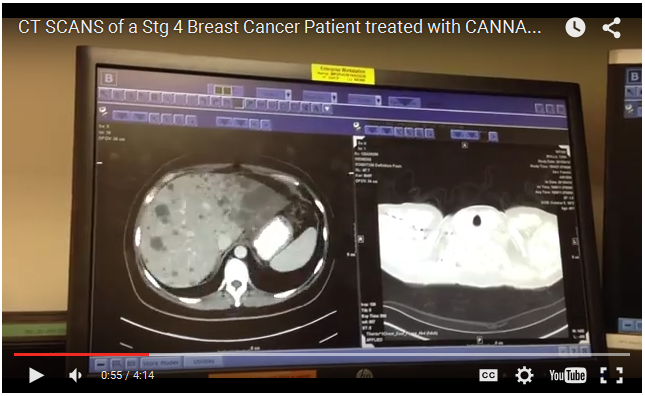
The second image (left side above), also part of the baseline study, shows the extensive liver involvement from metastatic disease. All of the small darker “spots” are metastatic lesions from the breast tumor.
Below is a close-up showing hundreds of liver mets. It is literally filled with metastatic disease. Usually when cancers have spread this far it’s hopeless to think of a cure.

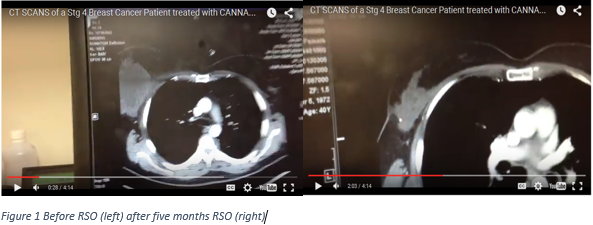
The following image (below) was taken in August of the same year five months after cannabis oil therapy. Note there is no mention as to how much cannabis oil she was taking, how long and how often are also unknown.

Compare the original breast lesion from the first image between nine and ten o’clock (below left) to the above image (provided again below right). You see a dramatic (that’s the term the oncologist used) shrinkage of the primary breast tumor.
The image seen below is a comparison of the liver involvement between baseline (left side) and canna-oil treatment (right side) after five months.
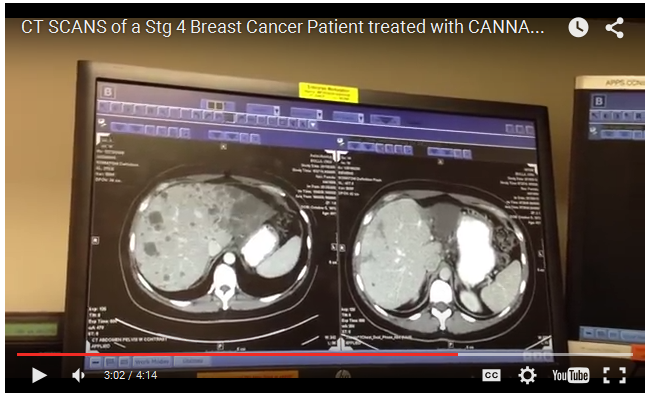
What is clear from this image is the literal disappearance of the darker grey liver mets replaced by what looks like normal, healthy liver parenchyma (smooth lighter grey regions). It appears that the RSO (and chemo?) has regenerated liver tissue. The larger mets have shrunk down to tiny nodules and the rest has disappeared-an astonishing response. Keep in mind that she was also taking another chemotherapeutic drug with the canna-oil.
As per the oncologist he mentions that it appears as if the liver mets have decreased in size further still. She had bone mets to the spine which have also disappeared. Her oncologist was obviously very pleased with the results.
Then things changed about one year later.
As of February 2014, an accident with unexpected seizure landed Cira in the emergency room a broken left shoulder and rib. Following her assessment an MRI determined there are now brain…metastasis (small brain tumors). Cira is faced with a challenging road ahead physically, mentally, and financially….[ref]IBID[/ref]
As is the case many times there is little follow up on what has happened since these CT scans were taken. The last Facebook entry was March 8, 2014. Sadly, it appears that she had died from complications of her cancer. What happened?
Although I am missing a lot of information we can initially see the unbelievable change in her status from riddled with tumors to nearly tumor free. Then something changed over the course of about a year. Was it due to a change in dosing? Or does this sort of thing happen with marijuana? Do patients sometimes achieve miraculous remissions only to have the cancer return with a vengeance? Maybe patients do better without chemo using only RSO?
No matter what happened we can still learn from this. We clearly see the effects of canna-oil and chemo together which was phenomenal. This case was particularly distressing to me for several reasons. One is that she had breast cancer which is running rampant across the planet and two is the shocking 180 turnaround after being nearly in remission! What a waste with such a beautiful and talented cinematographer. I only wish I had all of the information regarding this case.
Lastly, notice how nearly every case I present there is an element of financial ruin associated with it. In the wealthiest country in the world is this the best they can do?

The DEA and FDA are Conspiring to Suppress Cannabis Research
The DEA and FDA are Conspiring to Suppress Cannabis Research
By maintaining marijuana’s schedule I status for over 45 years the US government has been able to sustain the world-wide myth that marijuana is a drug of abuse, as addicting as heroin and medically worthless.
In a paper entitled: Ending the U.S. Government’s War on Medical Marijuana Research, the well-heeled Brookings Institute recently published their analysis suggesting that the War on Marijuana should end; that the controlled substances act uniquely orphaned marijuana into a no man’s land that forbade research.
Yet, of all the controlled substances that the federal government regulates, cannabis is treated in a unique manner in ways that specifically impede research.
THE CONTROLLED SUBSTANCES ACT
The nail in the cannabis coffin was finalized with the Controlled Substances Act (CSA) which fraudulently assigned marijuana schedule I drug status. Signed into law by President Richard Nixon as the Comprehensive Drug Abuse Prevention and Control Act of 1970.
Meanwhile, you might ponder that there has been a colossal change in the attitudes of our government officials over the last two decades after being schooled on the safety and health-giving properties of cannabis.
But you’d be wrong to consider that. As proof just a few weeks ago the new acting director of the DEA publicly admitted the obvious, that he felt marijuana was probably safer than heroin.
Predictably, Rosenberg did emphasize that he believed cannabis posed potential harms, stating: If you want me to say that marijuana’s not dangerous, I’m not going to say that because I think it is. Do I think it’s as dangerous as heroin? Probably not. I’m not an expert.[ref](http://blog.norml.org/2015/07/30/new-dea-leader-suspects-marijuana-is-not-as-bad-as-heroin/) 11/01/2015[/ref]
However, this statement was fired as damage control on the heels of an earlier awkward remark implying that pot and heroin were equally destructive.
Ok, you’re not an expert but you know for certain that marijuana is bad for you? In the same breath he blithely remarked that the leaf is what is smoked in cannabis.
When I first read these comments I had to laugh.
I immediately thought of Austin Powers when he was re-animated. Austin-stuck in the sixties-had no idea how much the world had changed. His remarks often times making him look hilariously absurd and antiquated. But Mr Powers had a serious excuse: he was cryogenically obtunded.
Not so with our DEA officials who seem always out of touch with the times and other government institutions. Liken our Drug Czar and DEA officials to suffering an Austin-like loss of perspective but without the gelato-festooned excuse.
This stems from a culture of prejudice against pot, marinated with an incapacity to change in the face of rapid scientific advancements. Over several decades compelling research has debunked the dogmatic paradigm of “weed is dangerous and as addicting as heroin.” Reflecting the massive amounts of new material that has accumulated that soundly countermands old-school, provincial notions of pot as a serious narcotic of abuse.
However, the scaffolding that has prevented pot from being recognized as a true medicine is still in place. Every attempt to remove these blockades has been met with frustration. From the Brookings Institute:
Historically, four petitions that have been initiated to reschedule marijuana or remove it from the schedules entirely have been denied or stalled by DEA with disposition times ranging from five to more than 20 years.
MEET THE NEW BOSS, SAME AS THE OLD BOSS
When you are foolish it’s best to stay quiet. That way the few that still respect you can pretend that you’re not. Moments after polishing his new tin badge he started his diatribe. The new DEA chief’s comments provide clinical proof that genius avoids bureaucracy.
Are you sitting down?
Mr Rosenberg stunned, and incensed, the world this week with his petulant comments that smoking pot as medicine is a joke.
Defying five-thousand years of cannabis medicine, insulting a half-dozen medical academies and 25 US state governors, while displaying text book Dunning-Kruger Effect, (a metacognitive inability of the unskilled to recognize their own ineptitude and evaluate their own ability accurately)[ref](https://en.wikipedia.org/wiki/Dunning%E2%80%93Kruger_effect) 11/07/2015[/ref], the new appointee embarrasses the US while spiralling into abject foolishness.
WHAT REALLY BOTHERS ME
Mr. Rosenberg, not unlike a Medieval Pope, and way too comfortable in his new skin, lets the world know what he thinks (sic) by going for the jugulars:
What really bothers me is the notion that marijuana is also medicinal — because it’s not,…We can have an intellectually honest debate about whether we should legalize something that is bad and dangerous, but don’t call it medicine — that is a joke.[ref](http://www.cbsnews.com/news/dea-chief-says-smoking-marijuana-as-medicine-is-a-joke/) 11/07/2015[/ref]
Like a bug solidified in amber, his comments reflect the DEAs prehistoric, refractory attitude toward marijuana. Especially now as Canada, Mexico, Jamaica, the world actually, are planning to legalize cannabis. It’s impertinent and pretty disheartening to those who suffer from illnesses for which cannabis supplies the only relief.
What really bothers me is his profound ignorance and incredible hubris. He just said that every state’s MMJ programs are a joke. That he alone knows better than all of the medical minds that have legislated marijuana into medicine. In just a few weeks he has already alienated half the population for saying that pot is as bad as heroin, that consumers smoke the leaf not the flowers of cannabis, and that it’s very dangerous without quoting a single study.
Why hire an adversary to surf the inevitable tidal wave of cannabis legalization?
We expected this with the stubbornly intractable former queen of the DEA.
MICHELE LEONHART
Mrs. Leonhart is more like a flu-dream aberration of our English hero King Richard the Lionheart who won the love and respect of his country from his successful military campaigns in Outremer during the Third Crusade.
Lacking much needed deference from the scientific community and the general public, she’s no novice when it comes to controversy. As former chief of the DEA one would assume that this person knew the potential harms of the illicit drugs she puts people in jail for. Yet some of the most oblivious comments on marijuana that any government official has ever claimed (save for Rosenberg) were routinely produced by Michele Leonhart.
Like Rosenberg, Leonhart’s atavistic ideas toward marijuana are based more in lore, legend, and magic than science. It displays the culture of bias Kool Aid our DEA officials wantonly guzzle.
Before stepping down in a storm of criticism (fired?) for allowing DEA agents to party with Columbian prostitutes in Cartel-funded sexcapades on her watch, she didn’t shy away from more controversy.
Leonhart’s inappropriate disapproval of Obama’s leniency toward marijuana activists after a 2012 meeting is revealing. Apparently she was infuriated that her boss used science and reason to formulate an opinion on pot’s harms.
IT’S LESS HARMFUL THAN BOOZE
President Obama stated factually that marijuana was less harmful than alcohol. Something any high school misanthrope would have to agree with even if he or she were budding neocons.
The New Yorker published an exclusive interview with Obama, in which he said marijuana is less harmful than alcohol and that “it’s important for [legalization] to go forward” in Colorado and Washington, whose residents voted in November 2012 to allow recreational use of the drug.[ref](http://www.usnews.com/news/articles/2014/01/27/dea-leader-fumes-about-white-house-playing-softball-with-marijuana-legalizers) 11/01/2015[/ref]
To appreciate how benighted her ilk are let’s look at this quote in reference to the statement made above by Mr Obama:
To have the president of the United States publicly say marijuana was a bad habit like alcohol was appalling to everyone in that room,” Kern County, Calif., Sheriff Donny Youngblood told the Herald. “I think the way that [Leonhart] felt was that it was a betrayal of what she does for the American people in enforcing our drug laws. … She got a standing ovation…
“I wasn’t there and can’t comment on what she said,” DEA spokesman Rusty Payne tells U.S. News, “[but] it shouldn’t be a surprise that we’re not for drug legalization…. That’s been consistent forever, so I don’t know if this is anything new or surprising.”[ref]IBID[/ref]
Pretty revealing…but appalling? Really?
Donny, was the standing ovation for NOT knowing the difference between marijuana and alcohol?
IT’S ALL BLACK AND WHITE
In the DEA criminal justice orbit there is no middle ground. Because of this ignorance they are often at odds with other fellow institutions, and the current administration’s philosophy and nearly all of the science.
Apparently, they don’t read much on the drugs they enforce and they don’t care. Armed with personal bias while citing irrelevant, poorly designed or outdated studies, they still insist that marijuana is harmful and of no medical benefit.
They wear the white hats and marijuana wears a black hat, very simple. Even when Obama disagrees with them they apparently do whatever they want to do.
That’s the definition of a rogue agency is it not?
DO WE STILL NEED A DEA?
This cultural mindset of ideology over science flows through the veins of these institutions in particular the DEA, but the FDA and NIDA don’t fall far from the tree.
Since marijuana is so harmful, they contend, only the penal system can correct the problem. So for the last forty-five years their solution was to put people in 10 x 10 cages for decades. Makes sense right? That’s DEA deductive reasoning (sic). Well done.
That’s why to this day we still must endure nearly 700,000 arrests per year for simple possession of marijuana in the US. Furthermore, it has led directly to 1,559,091 non-violent drug offenders behind bars. That’s one and one-half million people either in prison, on parole, or on probation who are victims of the drug war.[ref]NORML[/ref]
Now where’s that standing ovation?
FEDERAL PROSECUTORS ARE OFF THE RESERVATION
The new DEA acting director Mr Rosenberg is already proving to be worse than Leonhart. In direct violation of the spirit of the DOJs recent announcement, his agency busted three Indian Nations for growing marijuana or hemp.
Of course, the native American tribes involved only started grow operations AFTER the DOJ recently gave them permission to grow pot/hemp! Just this last fall the DOJ sent to all US attorneys the US Department of Justice Cole Memorandum Oct 28, 2014. It provides guidelines for Indian tribes with eight federal priorities to avoid such as distributing marijuana to minors, or preventing pot possession or use on federal property.
The latest casualty occurred with the Menomonee Indian reservation’s 30,000 plus cannabis operation in Wisconsin. After allowing both state and federal officials to tour the facility and take samples for analysis, the feds came back, not with reason, but with MP5s, scythes, hubris and plumes of cheap aftershave to destroy the fledgling grow site.
Meanwhile with a 30,000 pot plant investment mowed off the map the Menomonee Indians must endure the crippling debt the DEA left them with.
This just in (Nov 10, 2015): The Flandreau Santee Sioux Tribe of South Dakota who planned to open the world’s first pot resort in January is now on hold until further clarification comes from the DOJ. Thousands of pot plants have been destroyed as part of the negotiations.
Have these federal prosecutors gone off the reservation?
After all, the Menominee aren’t the only tribe to take the Justice Department at its word, only to be raided down the road. This past summer, the DEA raided two California tribes, the Pit River Tribe and the Alturas Indian Rancheria, seizing 12,000 plants.
Are the tribes being held to a different standard than states where it is legal?
Menominee Tribal Chairman Gary Besaw doesn’t know, but he isn’t happy about it.
I am deeply disappointed that the Obama administration has made the decision to utilize the full force of the DEA to raid our Tribe,..We offered to take any differences in the interpretation of the farm bill to federal court. Instead, the Obama administration sent agents to destroy our crop while allowing recreational marijuana in Colorado. I just wish the President would explain to tribes why we can’t grow industrial hemp like the states, and even more importantly, why we don’t deserve an opportunity to make our argument to a federal judge rather than having our community raided by the DEA?[ref](http://stopthedrugwar.org/taxonomy/term/159) 11/03/2015[/ref]
The betrayal of trust is in keeping with a 200-year tradition of breaking contracts with Indian nations.
In an interview with US News and World Report, tribal law expert Lance Morgan, a member of Nebraska’s Winnebago tribe who has worked with tribal governments pondering marijuana operations, said the Cole memorandum guidelines are not being applied consistently and warned the Menominee raid would be remembered as a historic betrayal.
How can you allow people to buy marijuana in a retail environment in some states and then raid an industrial hemp operation of a tribe? The only difference is that there is a tribe involved,…
This odd federal policy of encouraging investment and then raiding the new business sets us back a few decades in federal tribal trust and economic policy.[ref]IBID[/ref]
CONTROL RESEARCH
Another clever way to maintain marijuana’s “demon status” is to control who gets access to approval, funding, and pot cigarettes for any new study. A monopoly over approving academic study proposals while limiting the availability of medical marijuana for clinical studies in the US ensures that only very select applications receive a green light. Often times these studies are designed to make cannabis look bad.
It also ensures that the forward flow of scientific enquiry regarding marijuana’s astounding syllabus is choked to a capillary-like trickle.
Critics contend that the DEA, FDA, and NIDA maintain an ivory curtain of bureaucratic barriers to discourage any enthusiastic researcher from elucidating just how “medical” marijuana can be.
After all, we can’t have scholars contradicting the dangers of marijuana by revealing pot’s potential for curing disease.
That would make it a medicine which changes everything.
And that might embarrass some apex bureaucrat who’s underwhelming fund of knowledge on cannabis comes from his own agencies antediluvian pamphlets.
This has worked out exceedingly well for those in lofty government positions looking to protect their entrenched jobs designed to maintain the status quo.
Yet for every negative we also have the opposite. Take the inauguration of the first cannabis only research facility in the US.
THE BIRTH OF THE CMCR
In the year 1999 an agency was formed called the Center for Medicinal Cannabis Research (CMCR; www.cmcr.ucsd.edu). Their objective is to expand the public scientific knowledge on the therapeutic usages of marijuana. Their 2010 publication provides an illustration.
Below is a decision flow chart provided by the CMCR which demonstrates the complex interwoven hurdles clinicians must tolerate to receive approval for human studies in the USA.
Because of this imbroglio, we have very little human clinical peer-reviewed information on marijuana, and we desperately need double-blinded inquiry.
In their conclusions the CMCR had this to say:
As a result of the vision and foresight of the California State Legislature Medical Marijuana Research Act (SB847), the CMCR has successfully conducted the first clinical trials of smoked cannabis in the United States in more than 20 years. [Emphasis mine]
STEP BY STEP
Here’s how the labyrinthine process works or perhaps how and why it doesn’t work.
In order to evaluate the scientific validity of the proposals submitted, the CMCR engaged senior scientists from around the nation to serve as a Scientific Review Board (SRB). So far so good.
Studies recommended for funding by the SRB have to be approved by five different institutions/committees. That’s five committees and four too many.
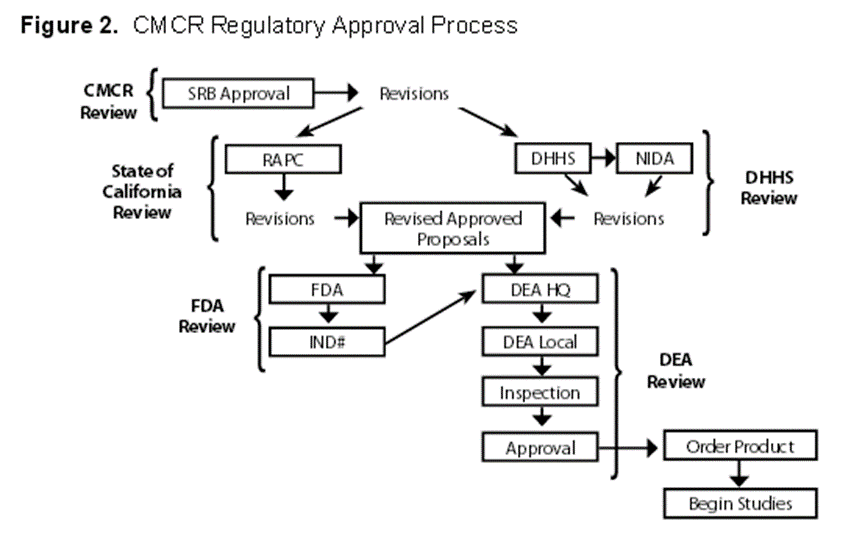
First the proposal is submitted for review to the Research Advisory Panel of California (RAP-C), followed by the Office of Public Health and Science of the federal Department of Health and Human Services (DHHS), the Food and Drug Administration (FDA), the National Institute on Drug Abuse (NIDA), and the Drug Enforcement Administration (DEA). [Note: approval from the DHHS is no longer required as of 2015]
Upon final approval from each of the above agencies, study teams were authorized to order cannabis cigarettes from NIDA and to begin recruiting patients. This process is described in Figures 1 and 2.
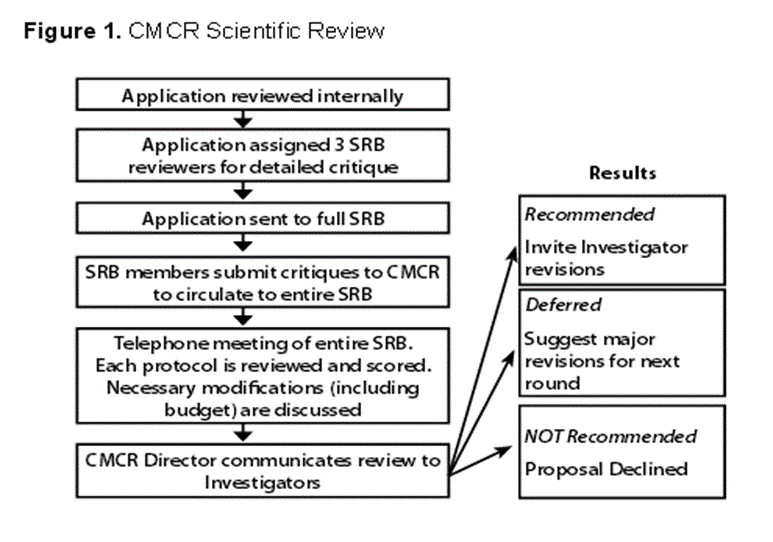
The impenetrable Byzantine-like application process, along with the deliberate blackballing of marijuana by government officials, is now the greatest impediment to learning the true nature of marijuana and its health benefits.
OLE MISS, POLITICS AND SCIENCE
Note in figure two the bottom right corner the box entitled “order product.” That refers to ordering research weed from NIDA. The only source for cannabis cigarettes for clinical study is through NIDA’s “Ole Miss” canna-plantation which has maintained a monopoly on medical cannabis for nearly five decades.
According to several researchers Ole Miss produces schwag with a hemp-like profile. Heavily criticized by scientists across the country the University of Mississippi’s marijuana product has been called into question for being weak, old, and as dried out as Gobi Desert sand biscuits.
When confronted with these underwhelming facts NIDA spokesperson Sheri Grabus said she has heard of no concerns about the quality of their cannabis product. She went on record saying that NIDA is satisfied with the University of Mississippi’s performance and subsequently renewed their monopoly.
The National Institute on Drug Abuse, a branch of the National Institutes of Health, administers the program and in late March granted Ole Miss a $68.7 million contract renewal, effectively upholding the university’s distinction as America’s legal weed supplier.[ref](http://www.ibtimes.com/how-mississippi-lab-taught-us-everything-we-know-about-marijuana-better-or-worse-1890470) 11/05/2015[/ref]
But Rick Doblin (see below) takes umbrage saying “It’s old, dried, brittle and mixed with seeds and stems. This has not been quality. Their goal is to provide poor quality medical marijuana to researchers in order to get negative results. Some of the marijuana is over ten years old.”[ref](https://www.mainstreet.com/article/governments-marijuana-contract-open-bids-nobody-reaches-it) 11/01/2015[/ref]
A quick gander on the NIDA website regarding THC content of their pot supply shows it to be remarkably feeble. The highest THC content available on the site was 6.7% for the high (sic) strength batch, with most of them running between 2% for low strength and up to 3.6% for medium strength. These numbers are more consistent with old Mexican brick marijuana than today’s varietals. Now add ten years of shelf life and the THC vanishes.
Many clinicians question whether the marijuana product Ole Miss is churning out each year can rightly be given medical status. A quick study of typical California medical grade pot versus “Ole Schwag” leaves one with a sense of despair.
Or compare this to Israel’s canna-plantations. The differences are disturbingly vast.
Using low potency marijuana is yet one more factor that can undermine clinical success in human trials.
CHANGE? NOT LIKELY
One person tried to change things up a bit. Dr. Lyle Craker, a professor at the University of Massachusetts filed a suit in 2001 to be allowed to grow research cannabis. Dr Craker said the quality from NIDA’s supplier, the University of Mississippi, was poor and the supply was constrained. After years of efforts, a DEA Administrative Law Judge approved the University of Massachusetts to grow the research cannabis, only to be overruled by the DEA.
Surprised?
Rick Doblin is the CEO of the Multidisciplinary Association for Psychedelic Studies (MAPS). He recently received approval to study the effects of marijuana on PTSD in US veterans using NIDA’s very own University of Mississippi pot supply. He stated in reference to the apparent shortage of marijuana for study,
NIDA is required under the Controlled Substances Act of 1970 to provide a ‘continuous and uninterrupted supply’ of marijuana for research, which they have now admitted to failing to provide.[ref](https://www.mainstreet.com/article/governments-marijuana-contract-open-bids-nobody-reaches-it) 11/01/2015[/ref]
When you add insufficient supply of marijuana to the list as yet another road block retarding clinical research, one is almost forced to concede that NIDA is deliberately shorting those who need pot cigarettes for their studies.
Think about it, if there are only a tiny body of researchers in the US utilizing Ole Miss for medicine (23 currently) where in creation is all of the marijuana going? They have twelve acres of pot plants located in the rolling hills of northeast Mississippi producing marijuana year after year with very few patrons using it.
Factor in the cultural bias that we have seen from above and it makes perfect sense why nothing gets done regarding weed research.
RESCHEDULE? FORGET ABOUT IT
What about rescheduling marijuana to a schedule II or III status? Like finding the Golden Fleece many have tried, all have failed. Four bills have been introduced, the first in 1981, that would either move marijuana to Schedule II or remove it from the schedule entirely. Each proposal has died in committee.[ref](http://www.brookings.edu/~/media/research/files/papers/2015/10/20-war-on-marijuana-research-hudak-wallack/ending-the-us-governments-war-on-medical-marijuana-research.pdf) 11/05/2015[/ref]
Don’t forget the waiting period which takes years. Perhaps the ultimate hurdle is wearing down the applicant to a point of capitulation; growing moss while waiting for a decision can be brutal.
Lastly, there exists a sticky wicket to launching your own grow facility should you desire to apply for the US contract next time. It’s another catch 22 which goes like this, as Rick Doblin explains:
You have to demonstrate [that] you have an FDA license to apply, which only Ol’ (sic) Miss has. It’s fruitless for anyone else to apply. If you currently cultivate marijuana, then the DEA says you are violating Federal law and therefore you can’t get an FDA license.[ref](https://www.mainstreet.com/article/governments-marijuana-contract-open-bids-nobody-reaches-it) 11/02/2015[/ref]
IN SUMMARY
The culture of bias in our antiquated, agenda-driven institutions, most notably the DEA, is the main reason why pot maintains the undeserved reputation it has had since the late 1950s.
I have listed over a half-dozen reasons why the situation will never change until our government abide by what its citizens demand by replacing intractable, calcified, anti-pot bureaucrats with more enlightened officials.
It’s a situation that is inexcusably the fault of federal policies failing to keep pace with changing societal views and state-level legal landscapes.[ref]John Hudak PhD, Grace Wallack. Brookings.edu (see number 12 above for link to PDF document).[/ref]
It will take time and a visionary president who is not afraid to use scientific reason over the ignorance and fear of marijuana that federal officials have maintained through bureaucratic folk lore.

Former Cancer Researcher Chooses Cannabis Over Chemotherapy, Treats His Prostate Cancer
Former Cancer Researcher Chooses Cannabis Over Chemotherapy, Treats His Prostate Cancer
I think we all need to pay attention when a cancer researcher refuses community standard chemoradiation, and instead opts for a schedule I drug with no medical value. Does he know something we don’t?
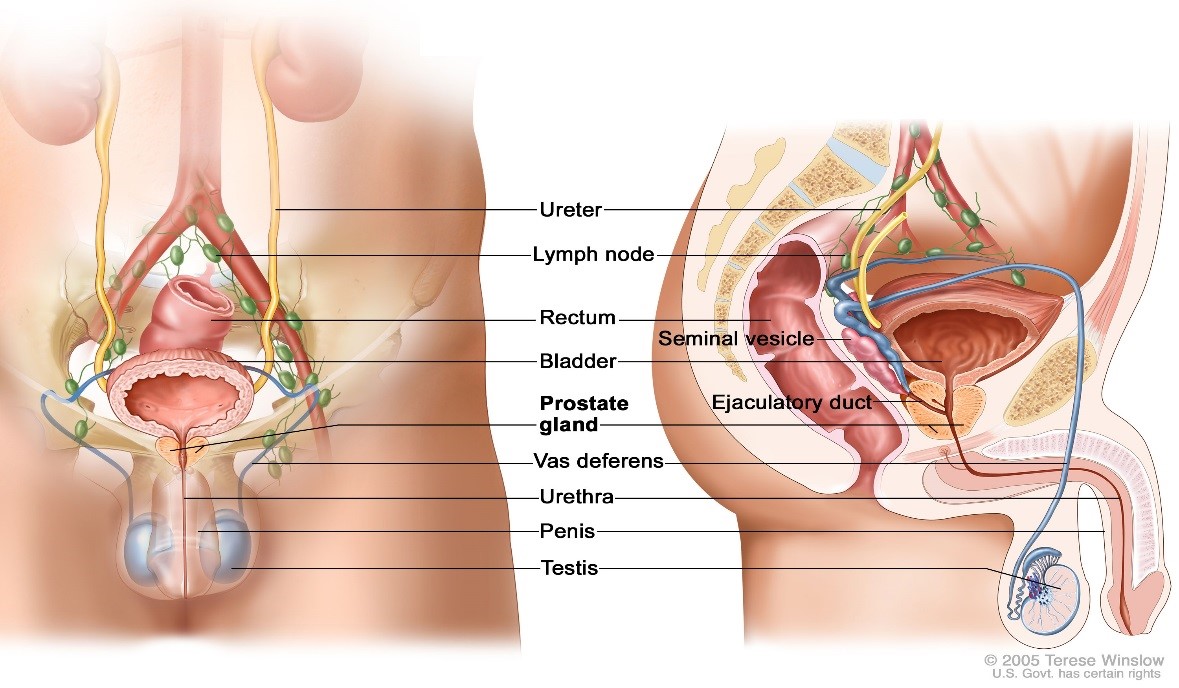
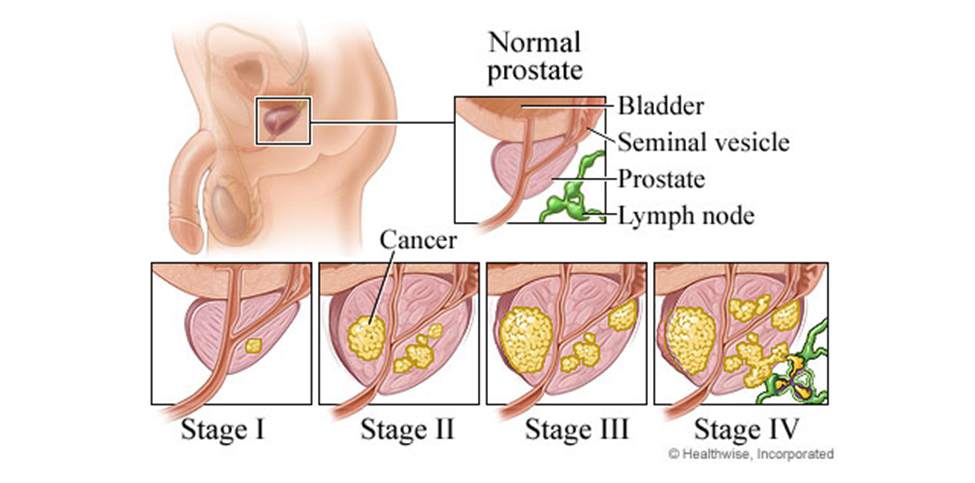
OVERVIEW OF PROSTATE CANCER
From the National Cancer Institute:
Prostate cancer is the most common cancer in men in the United States, after [non-melanoma] skin cancer. It is the second leading cause of death from cancer in men.
Almost all prostate cancers are adenocarcinomas (cancers that begin in cells that make and release mucus and other fluids). Prostate cancer often has no early symptoms. Advanced prostate cancer can cause men to urinate more often or have a weaker flow of urine, but these symptoms can also be caused by benign prostate conditions.
Prostate cancer usually grows very slowly. Most men with prostate cancer are older than 65 years and do not die from the disease. Finding and treating prostate cancer before symptoms occur may not improve health or help you live longer.
…Even with widespread screening with prostate-specific antigen (PSA), still 5% of cases present with metastatic lesions at the time of diagnosis. Because of all this, there is a fundamental necessity to search for and find new and novel treatments to this common pathology…. There has been experimental evidence that cannabinoids possess anti-androgenic [anti-testosterone effect which in theory should slow down or halt progression of the disease] proprieties…
In the United States, an estimated 217,730 cases will be diagnosed in 2010 and 32,050 deaths will occur [CA Cancer J Clin. 2010;60:277–300]…With testing localized disease incidence has increased while metastatic disease incidence has decreased.
Yet metastatic disease remains an important problem. Hematogenous [blood] spread of prostate cancer cells is a common event. For these malignant cells, tumor growth preferentially occurs in bones of the axial skeleton [the spine]. The most common site of metastasis is bone and frequently is symptomatic, causing pain, debility, and functional impairment.
The treatments differ depending on the presentation. With bone pain from metastatic involvement the usual choice is a chemical or physical castration called androgen deprivation therapy (ADT)
There are second line hormonal treatment if ADT fails.
Also there is external beam radiation therapy,…for men with castrate-resistant prostate cancer and bone pain that is limited to one or a few sites.[ref]Indian J Urol. 2012 Jan-Mar; 28(1): 9–14.[/ref]
ROLE OF CANNABINOIDS IN MALE PHYSIOLOGY
Previous research in the 1980’s has determined that the endocannabinoid system when stimulated, suppresses the male androgen [testosterone] response with a dose-dependent decrease in PSA [prostate specific antigen] expression and secreted PSA.
PSA is considered as the most sensitive biomarker and screening tool for prostate cancer to date; its regulation is androgen [testosterone and its derivatives]-dependent.[ref]IBID[/ref]
Current studies show that expression of both CB1 and CB2 receptors was significantly higher in cultured prostate cancer cells. When these cells were stimulated using a THC analogue (agonist, WIN-55,212-2) prostate cancer cells were encouraged to die off leaving normal cells untouched. These data suggest that both CB1 and CB2 receptors may be involved in [agonist] mediated growth inhibition and apoptosis [cell-mediated suicide].[ref]IBID[/ref]
The prostate gland when it undergoes malignant transformation, makes greater quantities of CB receptors on prostate tissue. This is the body’s compensatory response to the disease; to increase proliferation of CB receptors in an effort to fight off the neoplasia. It’s also an indication that prostate cancer may be yet another disease due to an endocannabinoid deficiency, adding it to the ever growing list of diseases for which this is the underlying pathophysiology.
It turns out that stimulation of CB receptors on prostate tissue induces prostate carcinoma cell (PCC) apoptosis [cell death], but cannabinoids other than Δ(9) -tetrahydrocannabinol (THC), which lack potency at cannabinoid receptors such as CBD have not been examined until 2013.
FROM ITALY
Cannabidiol (CBD) was first investigated (2013) by Dr L De Petrocellis and his team. Entitled Non-THC cannabinoids inhibit prostate carcinoma growth in vitro and in vivo: pro-apoptotic effects and underlying mechanisms.
They found that cannabidiol (CBD) significantly inhibited PCC viability.
This suggests the well known “entourage effect” is in play where several phytocannabinoids (or more) produce a synergistic effect each complimenting the other’s cancer-killing abilities and making the preparation much more potent and efficacious.
CONCLUSIONS AND IMPLICATIONS:
These data support the clinical testing of CBD against prostate carcinoma. In conclusion, the in vitro [test tube] data presented here allow us to suggest that non-THC cannabinoids, and CBD in particular, retard proliferation [growth] and cause apoptosis [cell death] of PCC (prostate carcinoma cells) via a combination of cannabinoid receptor-independent, cellular and molecular mechanisms. Indeed, the effects reported here, together with previously reported cannabinoid receptor-mediated effects of THC on PCCs, might encourage clinical studies on cannabinoids and Cannabis [sic] extracts as a therapy for human prostate carcinoma, either as single agent or in combination with existing compounds. Our additional observation that differentiation of an ‘androgen-dependent’ cell into a more malignant and ‘androgen-unresponsive’ phenotype increases its sensitivity to the pro-apoptotic effect of CBD might provide a new strategy to deal with the frequent loss of efficacy of AR [androgen receptor] antagonists against prostate carcinoma growth seen after only a few years of treatment.[ref]Br J Pharmacol. 2013 Jan; 168(1): 79–102[/ref]
Let me highlight this because it is actually quite profound. What they are saying in the last section is that cannabinoids perform better (are a more effective killing machine) on the worst type of PCC-the androgen unresponsive phenotype. These are the types that fail conventional drugs and are therefore much more deadly. Not so with cannabis apparently.
AMERICAN STUDIES
Probably the most famous prostate cancer patient is long-time “stoner comedian” Tommy Chong. Last year he reported that he was diagnosed with stage one prostate cancer. One year later he is presumably cancer free after his unconventional approach using cannabis oil, supplements, a healer, and a healthier diet.
After I came out with the news last June that a cancer doctor told me I had prostrate (sic) cancer… I immediately looked at alternatives. I contacted my nephew in Vancouver,…he suggested I meet with a Dr. McKinnon in Victoria, BC. That doctor changed my diet and put me on supplements, and within a year I brought my PSA numbers down drastically and eliminated the cancer threat. I also treated the condition with hemp oil (hash oil)…That’s right, I kicked cancer’s ass! So the magic plant does cure cancer with the right diet and supplements. I’m due for another blood test, MRI, etc., but I feel the best I’ve felt in years. And now for a celebration joint of the finest Kush…[ref](http://www.wakingtimes.com/2013/05/15/tommy-chong-beats-prostate-cancer-with-diet-and-hemp-oil/) 10/23/2015[/ref]
In reference to how he was able to easily obtain medical marijuana as a non-toxic, inexpensive alternative to toxic radiation and chemotherapy drugs, he had this to say:
I’ve got prostate cancer, and I’m treating it with hemp oil, with cannabis, so [legalizing marijuana] means a lot more to me than just being able to smoke a joint without being arrested.
Indeed. Legalization’s greatest effect will be to allow people dying from end-stage cancers to easily and legally obtain cannabis for making Rick Simpson Oil (RSO, hash/hemp oil).
DENNIS HILL
Dr. Dennis Hill is a PhD biochemist.[ref](https://patients4medicalmarijuana.wordpress.com/biochemist-dennis-hill-who-cured-his-stage-4-prostate-cancer-with-cannabis-oil-explains-how-it-works/) 10/25/2015[/ref] Dennis worked as a Cancer Researcher at the MD Anderson Cancer Center in Houston. Much to his surprise Dennis was diagnosed with advanced stage III prostate cancer. Stage III cancers invade local tissues which significantly increases mortality risk. Furthermore, as a researcher he often witnessed ineffective treatments for various cancers, he felt a new approach was in order.
Therefore, he decided upon RSO as the only form of treatment. He informed his doctor of the choice and surprisingly he didn’t object.
At first he experimented with cannabutter that a friend had, then switching to RSO for the Full Monty.
There was no dispensary in the area, but a friend made me cannabis butter, so I took that, up to tolerance. In three months the primary cancer was gone, only minor metastatic [stage III local invasion, not true metastatic disease which is stage IV] lesions were left. At that point I found a supplier for Rick Simpson oil and killed off the metastases in the next three months. Now I just take a maintenance dose of locally produced hash oil that is 1:1 THC:CBD with about a 30% potency. This will certainly keep me clear of cancer, anywhere, for ever.
My point in telling this story is the fact that in the face of advanced aggressive cancer, all I had was very weak cannabutter, but it was enough to eliminate the primary tumor. Now there are strains of 95% THC. But is this necessary? If you have cancer and want to pursue the cannabis treatment, any at all will be good. More important than extreme potency, is balance between THC and CBD. If you can get high potency, great. If not, common potencies will work perfectly.[ref]http://www.cureyourowncancer.org/dennis-hills-story-beating-prostate-cancer-with-cannabis-oil.html#sthash.J2KkKWUJ.dpuf[/ref]
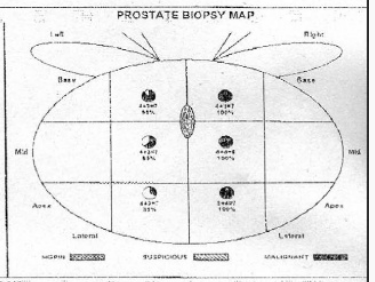
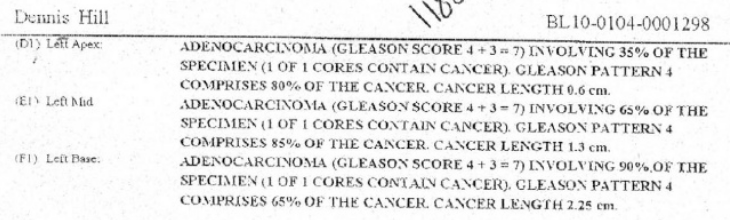
Above is Dr Hill’s biopsy schematic. In it we see six biopsy sites, all positive for adenocarcinoma (prostate cancer). Below is the pathology report for the left side. The right side is virtually the same.
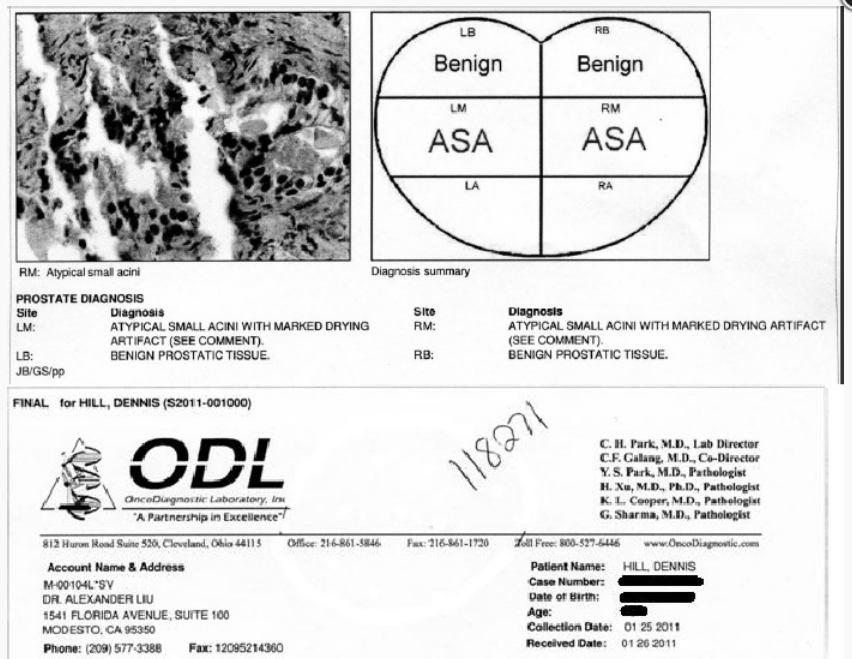
Below we have the follow up biopsy showing no active disease.
The Most Impressive Cannabis Case Study Ever? Treating Terminal Leukemia
The Most Impressive Cannabis Case Study Ever? Treating Terminal Leukemia
What I am about to show you is one of the most inspiring responses to the anti-tumoral actions of marijuana. It comes from the following case study provided by an Ontario oncologist. It clearly demonstrates in great detail how effective full-spectrum cannabis can be in treating one of the most pernicious forms of leukemia.
Normally this condition is approached using chemotherapeutic drugs, radiation, and/or a harrowing bone marrow (stem cell) transplant which entails great risk to the patient. Oncologists don’t like to admit it but these procedures can sometimes either kill the patient outright or leave them extremely debilitated.
One can almost always anticipate complications during a transplant since the patient’s leukemic bone marrow is “wiped out” with potent chemotherapeutics. Your bone marrow houses all of your immune cells. Patient with no immune cells for any period of time are extremely vulnerable to overwhelming infection.
In other words the treatment for this virulent form of ALL is often times as mortiferous as the disease itself.
FROM THE FAMOUS MAYO BROTHER CLINIC
Definition[ref](http://www.mayoclinic.org/diseases-conditions/acute-lymphocytic-leukemia/basics/alternative-medicine/con-20042915) 10/22/2015[/ref]
Acute lymphocytic leukemia (ALL) is a type of cancer of the blood and bone marrow — the spongy tissue inside bones where blood cells are made.
The word “acute” in acute lymphocytic leukemia comes from the fact that the disease progresses rapidly and creates immature blood cells, rather than mature ones. The word “lymphocytic” in acute lymphocytic leukemia refers to the white blood cells called lymphocytes, which ALL affects. Acute lymphocytic leukemia is also known as acute lymphoblastic leukemia.
Acute lymphocytic leukemia is the most common type of cancer in children, and treatments result in a good chance for a cure. Acute lymphocytic leukemia can also occur in adults, though the chance of a cure is greatly reduced.
The Treatments.
• Chemotherapy. Chemotherapy, which uses drugs to kill cancer cells, is typically used as an induction therapy for children and adults with acute lymphocytic leukemia.
• Targeted drug therapy. Targeted drugs attack specific abnormalities present in cancer cells that help them grow and thrive.
A certain abnormality called the Philadelphia chromosome is found in some people with acute lymphocytic leukemia. For these people, targeted drugs may be used to attack cells that contain that abnormality.
• Radiation therapy. Radiation therapy uses high-powered beams, such as X-rays, to kill cancer cells. If the cancer cells have spread to the central nervous system, your doctor may recommend radiation therapy.
• Stem cell transplant. A stem cell transplant may be used as consolidation therapy in people at high risk of relapse or for treating relapse when it occurs. This procedure allows someone with leukemia to re-establish healthy stem cells by replacing leukemic bone marrow with leukemia-free marrow from a healthy person.
A stem cell transplant begins with high doses of chemotherapy or radiation to destroy any leukemia-producing bone marrow. The marrow is then replaced by bone marrow from a compatible donor (allogeneic transplant).
Alternative medicine
No alternative treatments have been proved to cure acute lymphocytic leukemia.
Dear reader, one last thing to keep in mind: the below featured patient FAILED numerous highly toxic rounds of chemo and radiation. It did nothing for her cancer but it did harm her deeply putting the cannabis preparation’s foot to the fire.
In nearly every case I come across these end-stage patients are practically moribund before they earn the right to try something not on the hospital’s formulary. That needs to change.
So it’s even more impressive that the oil of cannabis succeeds in reducing her blast count when the most effective chemo fails. This miraculous accomplishment takes place right under their noses with a deaths-door patient severely ravished by chemoradiation.
THE CASE PRELIMINARIES
This is a case study involving a 14-year-old girl with the most aggressive form of acute lymphoblastic leukemia (ALL). It’s the Philadelphia chromosome positive form of ALL. This arrangement makes it very aggressive and difficult to treat.
These observations were first published in 2013 in the journal Case Reports in Oncology. In it the author documented a dramatic, and quite unexpected, dose-response decrease in her leukemic blast cell count due to the consumption of nothing else (at that time) but an extract of marijuana.
What I really liked about this published study is that it provides the reader with many of the details not seen when individual laypersons report their anecdotal responses to marijuana. Often times these circumstantial sagas leave me with more questions than they answer.
It’s refreshing to see a professionally compiled publication documenting the miraculous effects of pot with actual laboratory data. Even if it’s only one case the astonishing decrease seen in her “blast cell count” is unbelievable to say the least. This is one of the best-illustrated cases available in the literature.
THE APATHY
What still surprises me is how apathetic the media and drug companies are regarding bona fide cancer remissions using cannabis oil.
If canna-oil were a new investigational drug (able to be patented) we would see it featured as headline news in the Wall Street Journal and the New York Times as a “cure for ALL.”
Sadly this tactic may be the default reaction to canna-cures from the drug industry since the essential oil of cannabis is not a patentable “drug.” Drug companies prefer a patented synthetic analogue of just one component to make a magic bullet if you will. This alone will take an additional ten years on top of the ten years needed to study the essential oil in clinical applications.
Furthermore, it’s well documented that magic bullet cures for diseases, especially cancers, have never panned out the way the pharmaceutical houses had anticipated. Magic bullet cures for cancer simply do not exist even after forty-five years of R & D. But they keep going in that direction anyway. That’s the reason why chemotherapy is so popular-it makes lots of money for drug companies but it’s a crummy way to treat cancers.
That’s very disturbing to me when we have something that seems so remarkably effective and profoundly safe. Especially when we compare it to the deadly drugs currently on the formulary to treat this disease. Sadly the chemoradiation caused the premature death of this patient while the cannabis was curing her!
I think you’ll agree with me after you read the below study that no matter what the difficulties are in researching canna-oil, said studies need to be done ASAP because if anything is a magic bullet it’s cannabis oil.
THE CASE
The lead author Dr Yadvinder Singh commented in the introduction of his remarkable case report:
Cannabinoid resin extract is used as an effective treatment for ALL with a positive Philadelphia chromosome mutation and indications of dose-dependent disease control. The clinical observation in this study revealed a rapid dose-dependent correlation.
P. K., is a 14-year-old female resident of Ontario, Canada. In 2006 she presented with symptoms of weakness, shortness of breath, and bruising when she was taken to the Toronto Hospital for Sick Children on the 10th of March. There she was diagnosed with acute lymphoblastic leukemia (ALL), with >300,000 blast cells (immature leukemic cells) present in her blood.
After three years of unsuccessful chemoradiation and a failed stem cell transplant, she was deemed a conventional treatment failure. Numerous rounds of radiation and chemotherapy did nothing. A second bone marrow transplant was not recommended. She was subsequently placed in palliative home care essentially to die.
As such she was told by her oncologist to prepare for her disease to overwhelm her body and from which she would suffer a stroke within the next 2 months. Most likely she would die from the complications.
Like many of the resolute patients that you read about here the family wasn’t ready to roll over and accept a death sentence for their daughter. They decided on a move that thousands are calling a cancer cure.
WHO YOU GUNNA CALL? “CANCER BUSTERS”
RICK SIMPSON
While loudly singing “cancer busters” to the tune of Ghost Busters and steadfastly urged by her father’s research efforts, they decided to contact Rick Simpson the legendary architect of Rick Simpson Oil (RSO). RSO is an essential oil of cannabis extracted, in this case, with 99% isopropyl alcohol. RSO is becoming mythical in the lay communities for healing dozens of disparate diseases and driving numerous deadly cancers into remission. Even the professional community is taking notice-finally. The strain used was called Chronic, a hybrid of Northern Lights and several other hybrids such as AK-47.
DOSING RSO
The proper way to dose this material is to start off by eating a super-tiny amount and wait a few hours to see where it takes you. Remember this preparation is full-spectrum meaning that it is loaded to the gills with a very high percentage of THC. The idea is to start slow and increase at a pace you or your cancer determines.
For example, if you are riddled with metastatic disease you cannot afford the luxury of time so you’ll increase your dosing quantity very quickly-let’s say in two to three days. Others who have some time may take a week or longer to achieve the coveted one gram per day level.
The anti-cancer dose that most caregivers are satisfied with is orally taking a gram of RSO per day divided into three or four doses. One gram is roughly one ml on the graphs shown below.
She started out in the prescribed fashion by ingesting a tiny half-grain of rice size of the potent elixir. That was day zero. See the below graph in which her oncologist plotted the effects of cannabis versus blast cell count (BCC) and dose in milliliters of RSO.
View the BCC as a marker for ALL. When the BCC drops her disease is losing its foothold on her. As it approaches zero she is in remission. From the graph we see that she had an extremely high blast count peaking at 374,000 which normally would keep rising.
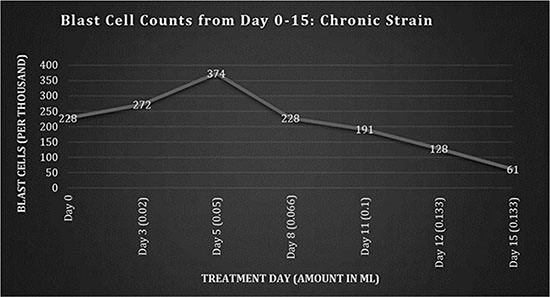
However, by day eight she was rapidly responding to the anti-tumoral actions of marijuana resin as she gradually built up a tolerance to the RSO and was able to increase her dosing.
Initially she had a tough time taking the potently psychoactive RSO. Even with tiny doses she reported several panic attacks along with increased appetite and fatigue.
The panic attacks may be due to the strain chosen which had some Sativa hybrids in it. Usually Mr Simpson and others who use this medication prefer to stick with the Indicas which tend to make you sleepy rather than stimulated. This helps you avoid panic attacks and anxiety while allowing you to dose higher. The Indicas encourage sleep to help heal.
After day 15 the original Chronic strain RSO was consumed to be replaced by a new (unknown) strain for the next round of dosing. As you can see from the below graph her blast count started to rise again doubling by day 27 to 66,000. Right at this point the dosing was increased from 0.5 ml on day 25; to 0.75 ml on day 27; and finally to 0.8 ml by day 34.

Then something very interesting happened. Her blast cell count suddenly plummeted to 6.9 by day 32. Meanwhile, some additional blood chemistries revealed that her uric acid levels were through the roof which started to produce joint aches and pains. Similar to acquiring the disease gout she was successfully treated pharmaceutically with allopurinol.
TUMOR LYSIS SYNDROME
But the fascinating thing is that all of the uric acid, her doctors determined, was coming from “tumor lysis syndrome.” This indicates that the cannabis preparation was so potent that it was killing off her blast cells with unheard of efficiency leaving her body to deal with the biochemical debris (uric acid) from an exponential die-off of cancer cells.
In fact, the cancer-killing effects were more dramatic than any known chemotherapy drug and hugely successful in treating her ALL. She was aggressively driving her ALL into remission.
HEMP OIL #3
On day 43, a new batch of hemp oil from an Afghan/Thai strain (referred to as Hemp Oil #3) prepared by the family was administered.
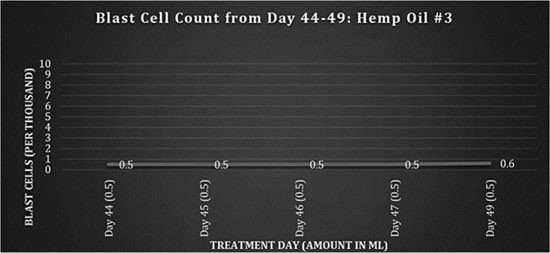
Above you can see the very low titer of blast cells showing how effective the preparation was. At this point she was essentially in remission with a fraction of the blast cells she previously had.
HEMP OIL #4
At around day 50 a new RSO formula was used. Keep in mind that the chemo drugs she was previously given only made her sick, malnourished, and vulnerable to infections. Due to the cataclysmic effects of the chemo she was not able to take foods orally during this period.
Several complications from her previous chemoradiation emerged. Since she was constantly nauseated and unable to keep food down she needed to be on TPN (feeding through an IV) to prevent further malnourishment. In light of the difficulties regarding oral feeding her dosing of RSO was decreased from three times per day to two. That change led to an increase in her blast count. Note that at times she was only receiving half of the recommended one gram of RSO per day. This was a terrible mistake.
Dr Singh:
The dosing regimen was intermittent until day 59, remaining at 1-2 doses per day of 0.5 ml. As the blast cells began to increase and the patient’s appetite increased, the dosing frequency was again increased to 3 times per day starting on day 62, and the amount administered was increased from day 65.
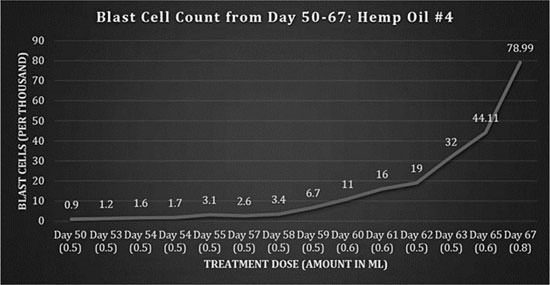
HEMP OIL #5
On day 68, a new batch of medicine was obtained by the family referred to as Hemp Oil #5. As you can clearly see there is a powerful dose-response decrease in her blast count, once again demonstrating that it is from the “hemp” oil and not a coincidence.
Also during the 78 days of RSO she was taking absolutely no other anti-cancer medications. Her doctor confirmed that this was not a spontaneous remission but due to the ingestion of cannabis essential oil. This is similar to a re-challenge effect where a medicine is stopped allowed to clear and then restarted to ascertain its true efficacy. It appears that the increased dosing of the RSO is responsible for this turnaround.
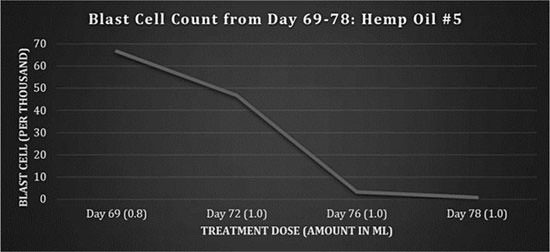
Lastly, we have the graph featured below which is a summary of the entire 78 days she was on RSO.
Although much more research is needed this graph clearly offers “proof” of efficacy even to steadfastly conservative mainstream oncologists who are very hostile to using “unproven” (err unpatented) drugs.
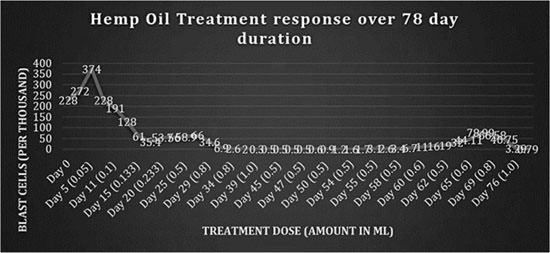
I am curious, would the outcome have been better had she refused chemoradiation or a bone marrow transplant? Even the author admits that the chemo substantially harmed her and led to her death. I suspect that she would still be alive today if she had only used RSO at the correct dose, and began her treatments the week she was diagnosed with ALL.
The previous chemoradiation had such an appalling effect on her health that she was never able to recover from it. The conventional treatments, and the disease, led to a severe neutropenia: a scarcity of an important immune cell line called neutrophils. These cells are the first to arrive when a patient develops an infection which ultimately caused in her case a bowel perforation, peritonitis, sepsis and death.
Often times in cases like this the oncologists wait far too long before trying cannabis oil.
Dr Singh:
This therapy has to be viewed as polytherapy, as many cannabinoids within the resinous extract have demonstrated targeted, antiproliferative [not able to reproduce], proapoptotic [inducing cell death] and antiangiogenic [halts new blood vessel growth in tumors] properties. This also needs to be explored further, as there is potential that cannabinoids might show selectivity when attacking cancer cells, thereby reducing the widespread cytotoxic effects of conventional chemotherapeutic agents. It must be noted that where our most advanced chemotherapeutic agents had failed to control the blast counts and had devastating side effects that ultimately resulted in the death of the patient, the cannabinoid therapy had no toxic side effects and only psychosomatic properties, with an increase in the patient’s vitality.
Another important point: as you can see from the above data the patient’s RSO formula was different each time they made a new batch. This is dreadfully inconsistent. Ideally we want one type of RSO made from the same varietal or at least the same species (Indica) each time.
UNDERDOSED?
Based on the graphs presented, the patient’s daily dose is indicated in parenthesis in milliliters on the horizontal coordinate. Although from the discussion versus the graphs it is not entirely clear what she received each day, we’ll have to assume that the amount in parenthesis is the total daily dose. If it is then she never received the recommended total dose of one gram (approximately one milliliter) per day for much of her stay.
Only on day 29 did she start to receive (close to) one gram per day total until day 39. The dose was decreased again by day 44. Then only the final 12 days did they return to 0.8-1.0 ml dose.
Increasing the dose in response to an increasing blast count and then decreasing it as the count drops was a bad idea.
CONCLUSION
Yet, in spite of an inconsistent black market pot supply and the likely underdosing, the results speak for themselves. With odds incredibly stacked against this brave young soul she nearly cured herself!
In fact, she did “cure” her ALL but the chemoradiation had destroyed her ability to recover.
What we have here is a crude weed extract made from a half-dozen differing varietals that any cave dweller could make blindfolded with one arm. Although it was probably full of impurities and differed in potency from batch to batch, we just witnessed an event that made the multi-billion dollar chemoradiation franchise look like a Keebler Elves bake sale.
IS ANYONE LISTENING?
Why isn’t this making front-page news around the world?
Clearly, for every critic to see with real data graphs, the anti-cancer activities of RSO are far more efficacious than the best chemo they offer. Plus it isn’t going to kill you to cure you. Think about this for a minute: a crude pot extract did this.
Now where does that leave us?
Well, we have a non-toxic drug that works overnight to kill blast cells, and it put ALL into remission in a matter of weeks.
If that’s not a magic bullet then I don’t know what is.

Latest Cannabis Research Update: Bladder Cancer, Israeli Studies and Anti-Tumour Properties
Latest Cannabis Research Update: Bladder Cancer, Israeli Studies and Anti-Tumour Properties
The Economist:
If (Marijuana) were unknown, its discovery would no doubt be hailed as a medical breakthrough. Scientists would praise its potential for treating everything from pain to cancer and marvel at its rich pharmacopoeia; many of whose chemicals mimic vital molecules in the human body.
Well said. If marijuana weren’t tarnished by its ability to make people happy, and its subsequent criminal underpinnings, we would be enjoying all of its favorable qualities, including treating stubborn diseases which modern medicine is tripping over to find cures.
In a previous segment I discussed the miraculous cannabis-cures of several patients with a deadly form of brain cancer called glioblastoma multiforme (GBM). In this segment I will update the reader on some of the latest political moves, cannabis research on cancer and other diseases across the globe.
GOOD NEWS
First on the American front we have a tiny bit of respectable news. In a 180 turnaround President Obama announced the intention to scrap one of the three titanic impediments to clinical investigations of marijuana in the US.
In 2015 Obama ordered that the US Public Health Service (PHS) is no longer needed for approval of research using cannabis on human subjects. Cannabis activists are rejoicing that researchers have one less hurdle to jump over.
In a bold and welcomed move Obama has eliminated one-third of the monolithic obstruction to marijuana research in this country. Previously clinicians had to receive approval from three government institutions before granting permission to use pot for human studies; historically all three, the FDA, the DEA and the USPHS, must rubber stamp applications for ANY study using medical cannabis.
Calling them redundant the Department of Health and Human Services reported the committee’s conclusions which:
…will help facilitate further research to advance our understanding about the health risks and any potential benefits of medications using marijuana or its components or derivatives.
By removing this boat anchor researchers think it will significantly improve the glacial turnaround times which can take years for application approval involving human and animal studies using marijuana.
There are still two huge roadblocks in place however. They are the FDA and the DEA. Both have been accused of having a “culture of criminology” and derailing research attempts using cannabis in treating human illnesses. All three have been known to drag out applications for years.
ORPHAN DRUG STATUS CBD
Meanwhile, last year the FDA granted Insys Pharmaceuticals orphan drug status to its pharmaceutical cannabidiol (CBD), for the treatment of glioblastoma multiforme (GBM). Glioblastoma multiforme is the most common and aggressive form of malignant primary brain tumor.
Orphan drug status has already been granted to Insys using their pharmaceutical CBD for treating Dravet syndrome (a rare form of intractable epilepsy that commences in infancy) and Lennox-Gastaut syndrome (a rare form of pediatric epilepsy).[ref](http://finance.yahoo.com/news/insys-therapeutics-cannabidiol-gets-orphan-193003258.html) 10/12/2015[/ref]
The company is looking into other applications which include adult epilepsy, chemotherapy-induced peripheral neuropathy and addiction in cocaine, amphetamines and opioids. Insys expects to seek orphan drug status for these additional indications if they qualify.
Orphan drug status grants pharmaceutical companies special financial incentives to develop the drug. This can only be good news as it furthers progression of much needed clinical trials using marijuana or one of its phytocannabinoids.
ISRAELI STUDIES
PURE CBD IN TREATING SOLID TUMORS
Once again if you are looking for human research using cannabis Israel is a good starting point. Hadassah Medical Organization has a new study proposed.
The Study: Pure CBD as Single-agent for Solid Tumor. In the application they state:
Increasing lines of evidence support an antitumourigenic effect of cannabinoids, including the cannabidiol (CBD) which does not posses [sic] the psychotropic effects of D9-tetrahydrocannabinol (THC). These include anti-proliferative and pro-apoptotic effects and they are known to interfere with several mechanisms in the tumorgenesis. Yet, evidence from clinical trials among cancer patients is needed. The aim of the current study is to evaluate the impact of CBD as single treatment among cancer patients.
The study is still in its infancy and not yet open for participant recruitment. More on the status of this trial as things progress.
IN VITRO ANTI-TUMOR ACTIVITY OF CANNABIS VARIETALS.
Another study was recently published and reported on in the Israeli daily Haaretz. It involved a preliminary study conducted by Israeli scientists who have discovered that cannabis may help slow the growth of certain cancerous tumors, even eliminating them completely.
The Israeli study was published this year (2015) by the cannabis friendly Israel Institute of Technology known as Technion. The main author Dr Meiri organized an on-going experiment involving 50 different Israeli-produced varietals of cannabis and over 200 cancer cell lines.
Dr. David Meiri, assistant professor in the biology department at the Technion, is leading the research team. The project began a year ago and is focused on the cytoskeleton and cell division in healthy and cancerous cells.
Dr Meiri:
There is a large body of scientific data which indicates that cannabinoids specifically inhibit cancer cell growth and promote cancer cell death,…In addition to active cannabinoids, cannabis plants also contain a multitude of other therapeutic agents, such as terpenoids and flavonoids that are usually present in small quantities, but can have beneficial therapeutic effects, especially as synergistic compounds to cannabinoids.[ref](http://www.i24news.tv/en/news/israel/society/67341-150411-israeli-study-finds-cannabis-delays-cancer-development) 10/11/2015[/ref]
Meiri and his team are documenting the cancer killing effects of cannabis preparations on brain tumors with fascinating results. They are witnessing marijuana’s ability to induce programmed cell death in cancer cells while leaving healthy cells alone. They have found similar effects on breast cancer cell lines.
MARIJUANA MAY LOWER BLADDER CANCER RISK
Back in America researchers at Kaiser Permanente in California published their findings regarding marijuana smoking and its relationship to bladder cancer. What they found was very interesting.
By analyzing their impressively large database of patients researchers uncovered a curious association. They found that pot smokers were 45% less likely to be diagnosed with bladder cancer than patients who did not smoke at all.
It’s very exciting because bladder cancer is hard to treat,” said Anil Thomas, MD, a urologist at the Southern California Permanente Medical Group. But he cautioned that the study does not prove that smoking marijuana prevents bladder cancer, and more research is needed to explore the connection.[ref](http://www.medscape.com/viewarticle/803983) 10/18/2015[/ref]
Dr Thomas presented his findings at the American Urological Association annual scientific meeting in 2013.
Dr Thomas: we know that tobacco smoking is the best established risk factor for bladder cancer, Dr. Thomas told reporters attending a news conference. But to date, there are no epidemiologic studies accurately characterizing the association between cannabis use and bladder cancer.
They analyzed over 82 thousand patient files from 2002-2003. Participants were between 45-69 years old. Here’s what they found:
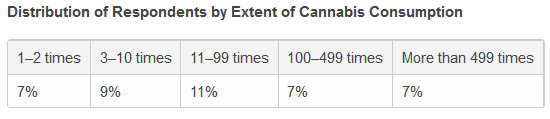
In all, 41% reported using cannabis, 57% reported using tobacco, and 27% reported using both. As predicted those who only used tobacco had an increased risk for bladder cancer.
Even more interesting is what happens to those who smoke both tobacco and marijuana. Those who partook of both had the same risk as those who used neither. Those that only smoked pot enjoyed a hugely significant decrease in risk for bladder cancer.
It appears that pot may offer some sort of protection from the toxicity of tobacco. This is not the first time I have seen this protective effect. We see it also in lung cancer studies with pot smokers where pot protects the lungs from the combustion products of tobacco.
Remember that these observations show associations and not causations. Therefore we cannot say with confidence that pot “caused” a reduction in bladder cancer. For that we’ll need further research but once again the epidemiology certainly looks good.
Dr. Thomas told Medscape Medical News that he first got interested in exploring this topic while doing some laboratory work in which he exposed prostate cancer cells and bladder cancer cells to cannabis.
“The prostate cancer cells did not show an effect and the bladder cancer cells were devastated,” he said.[ref]IBID[/ref]
Cannabis Shrinks Aggressive Brain Tumors - MRI Evidence of 3 Recent Case Studies
Cannabis Shrinks Aggressive Brain Tumors – MRI Evidence of 3 Recent Case Studies
Part One – The Worldwide Escalation of Cancers
At the risk of sounding Pollyanna I believe that the essential oil of cannabis may indeed be a “cure” for several diverse cancers once the dosing and other details are worked out. While I take care not to call it a panacea there are simply far too many cases of incredible remissions from seemingly incurable cancers to ignore these reports.
We are running out of time with our “war on cancer.” Experts agree that conventional approaches using drugs and radiation are a failure in treating most deadly cancers. Except of course for the National Cancer Institute and the American Cancer Society (see below Dr Epstein) who maintain the illusion of progress.
That means we need to determine if cannabis is the winner we all hope it will be. But before that happens we desperately need more human clinical research to prove the claims that cannabis cures cancer. While we pensively wait for that work to be accomplished, I’ll present several astonishing cases for you to examine.
Catch 22
Right now we find ourselves in an absurd catch 22: the FDA and the DEA have been telling us for forty years that they need more clinical research to prove the medical value of marijuana before it can be removed from its schedule I status. However, before we can obtain valuable clinical research on humans to help remove it from its prohibitive schedule I status, pot must be removed from its current prohibitive schedule I status so that human clinical trials may be undertaken. I feel a migraine coming on, what a mess!
Explosive Growth
Meanwhile the media and our medical academies have been curiously silent on the explosion of new cancer cases seen each year both in the US and abroad. In case you didn’t know, the documented incidence of cancer (all cancers combined) is increasing at a disturbing rate. This is particularly true for many of our deadliest cancers. While the rates escalate successful treatments have not. The death rates for the most deadly forms of cancer such as ovarian, pancreatic or glioblastoma have not significantly budged for 40 years.
Novelty Gone Wild
A hundred years ago cancer was a novelty. For example the US total number of lung cancer cases reported in the year 1900 was about 140. Yes, only 140 cases TOTAL. But over the last century it has become a major culling force. Up from a rare group of disorders to affecting one in three several years ago (US and Canada). Finally, as of 2015, American men stand a one in two chance of getting some kind of cancer in their lifetimes. A one in two chance, fifty-fifty. Women are not far behind. That’s astonishing when cancers like these were as rare as teeth on a drake mallard just a generation ago.
Dr. Epstein: Canary in a Coal Mine
We’ve been warned for decades by prominent academic scholars that cancers are running out of control. Much of this shocking news has been revealed to us in award-winning publications by Emeritus Professor Dr Samuel Epstein. His newest tome “Cancer-Gate: How to Win the Losing War on Cancer” is a groundbreaking new book.
It warns that, contrary to three decades of promises, we are losing the winnable war against cancer, and that the hand-in-glove generals of the federal National Cancer Institute (NCI) and the private “”nonprofit”” American Cancer Society (ACS) have betrayed us. These institutions, Epstein alleges, have spent tens of billions of taxpayer and charity dollars primarily targeting silver-bullet cures, strategies that have largely failed, while virtually ignoring strategies for preventing cancer in the first place. As a result, cancer rates have escalated to epidemic proportions, now striking nearly one in every two men, and more than one in every three women. This translates into approximately 50 percent more cancer in men, and 20 percent more cancer in women over the course of just one generation. [ref](http://www.amazon.com/gp/product/0895033542?*Version*=1&*entries*=0) 10/05/201[/ref]
In other words, as best-selling author Dr Abramson (Overdosed America) claims, we have lost the “War on Cancer.” The age-adjusted death rate for cancers overall is the same as it was in 1971. This means that should you find yourself diagnosed with an aggressive form of cancer you will need to think long and hard about your options. One option is to reject conventional approaches and reach for the hash oil especially if you are diagnosed with a brain tumor.
Glioblastoma Multiforme; The Deadliest of All
When I was in medical school studying neurology I recall one of my professors mentioning a dreadful brain cancer. It’s called glioblastoma multiforme (GBM). It stuck in my brain (pun intended) as the one cancer you certainly do not want; as if there are some that we do want?
My professor glibly stated that once diagnosed the patient will have just enough time to sort out their affairs before saying goodbye. Along with dozens of other deadly cancers rising like dandelions in the spring, GBM is more bite than bark and impossible to treat. Nothing in conventional medicine offers hope; neither chemotherapy, radiation, nor surgery can alter its fatal course. That’s why when I heard of people curing themselves with a marijuana concentrate I had to take notice.
Recall GBM’s most famous patient: the late senator Edward Kennedy. He predictably presented with a new onset seizure and was dead a few months later after “state of the art” cancer care from the eminent Duke University Medical Center.
From the American Brain tumor Association:
Glioblastomas (GBM)…These tumors are usually highly malignant (cancerous) because the cells reproduce quickly and they are supported by a large network of blood vessels.
Glioblastoma can be difficult to treat because the tumors contain so many different types of cells. Some cells may respond well to certain therapies, while others may not be affected at all. This is why the treatment plan for glioblastoma may combine several approaches. [Surgery, chemo and radiation]
…With standard treatment, median survival for adults with an anaplastic astrocytoma is about two to three years. For adults with more aggressive glioblastoma, treated with concurrent temozolamide and radiation therapy, median survival is about 14.6 months and two-year survival is 30%. However, a 2009 study reported that almost 10% of patients with glioblastoma may live five years or longer.
Children with high-grade tumors (grades III and IV) tend to do better than adults; five-year survival for children is about 25%.[ref](http://www.abta.org/brain-tumor-information/types-of-tumors/glioblastoma.html) 10/06/2015[/ref]
To summarize between 75% (children) and 90% (adults) are dead in five years.
According to the New England Journal of Medicine, GBM accounts for approximately 50% of the 22,500 new cases of brain cancer diagnosed in the United States each year. Treatment options are limited and expected survival is a little over one year.[ref](http://www.prnewswire.com/news-releases/gw-pharmaceuticals-commences-phase-1b2a-clinical-trial-for-the-treatment-of-glioblastoma-multiforme-gbm-231391971) 10/12/2015[/ref]
The Good News
It turns out that GBM tumors, like many others, are rife with cannabinoid (CB) receptors. Compelling evidence suggests that cancer cells littered with CB receptors respond well to full-spectrum cannabis preparations. The actions on these receptors from THC provides a valuable model to help explain the function of the phytocannabinoids in shrinking brain tumors.
In November of 2014 an article was published in Molecular Cancer Therapeutics which supported this concept entitled: The Combination of Cannabidiol and Δ9-Tetrahydrocannabinol Enhances the Anticancer Effects of Radiation in an Orthotopic Murine Glioma Model, by Katherine A. Scott, Angus G. Dalgleish, and Wai M. Liu. Department of Oncology, St George’s University of London.
Dr. Liu
In a Washington Post interview with Dr Wai Liu, he describes the results of their groundbreaking discovery in which cannabinoids could play a significant role in treating one of the most aggressive cancers in adults and children.
Dr Liu:
There are more than 85 cannabinoids, which are known to bind to unique receptors in cells and which receive outside chemical signals. These receptors feed into signaling pathways, telling cells what to do. Recent studies have shown that some cannabinoids have potent anti-cancer action. For example, both THC and CBD have been shown in a number of laboratory studies to effectively induce cell death in tumor cells by modifying the faulty signaling pathways inside these cells. Depending on the cell type, this can disrupt tumor growth or start to kill it.
The psychoactivity associated with some cannabinoids, principally THC (which gives people a cannabis high), is also mediated via the same receptors. Because these receptors are found in the highest abundances in brain cells, it follows that brain tumors also rich in these receptors may respond best to cannabinoids.
Depending on the individual, treatment can consist of surgery, radiotherapy, and/or chemotherapy with the drug temozolomide. However, due primarily to the intricate localization of the tumor in the brain and its invasive behavior, these treatments remain largely unsuccessful.
However, as our study showed, combining radiotherapy with cannabinoid treatment had a big effect.[ref](https://www.washingtonpost.com/posteverything/wp/2014/11/18/how-pot-helped-shrink-one-of-the-most-aggressive-brain-cancers/) 10/06/2015[/ref]
The big effect seen was when THC and CBD were combined it lead to a favorable and powerful antitumor effect achieving a 50% kill rate of test-tube glioma cells at half the concentration of either substance used alone.
In other words the synergistic effects of combined THC and CBD were far superior to either one alone. But each one had powerful antitumor effects on their own.
Once this information was established Dr Liu then tested the impact of combining the cannabinoids in special ratios with irradiation in mice with glioma.
Dr Liu:
But the secret to successfully exploiting cannabinoids as a treatment for cancer is to balance the desired anti-cancer effects with the less desirable psychoactive effects. This is possible, as some cannabinoids seem to function independently of the receptors and so do not engage the adverse effects. CBD is one such cannabinoid. The doses of THC we selected were below the psychoactive level, but together with CBD it partnered well to give the best overall anti-cancer effect.
THC, CBD And Low Dose Radiation
After trial and error they found that the very best approach used CBD, low concentrations of THC and low-dose radiotherapy.
Our results showed that the dose of irradiation we used had no dramatic effect on tumor growth, whereas CBD and THC administered together marginally reduced tumor progression. However, combining the cannabinoids with irradiation further impeded the rate at which tumor growth progressed and was virtually stagnant throughout the course of the treatment. Correspondingly, tumor sizes on the final day of the study were significantly smaller in these subjects compared with any of the others.
The results are promising. There may be other applications, but for now, it could provide a way of breaking through glioma and saving more lives.
THC, CBD And TMZ
A Combined Preclinical Therapy of Cannabinoids and Temozolomide against Glioma, Sofía Torres et al.[ref]Mol Cancer Ther January 2011 10; 90[/ref]
A Spanish research team headed by Dr Torres found that cannabinoid receptor agonists like THC the major active ingredient of marijuana, and other cannabinoid receptor agonists inhibit tumor growth in animal models of cancer, including glioma, an effect that relies, at least in part, on the stimulation of autophagy-mediated apoptosis-a type of suicide for tumor cells.
What they found was when THC was combined with the only known drug that is partially helpful in treating GBM, temozolomide (TMZ), had a powerful anti-tumor effect on glioma cells even if the cells were resistant to TMZ alone. THC somehow induces autophagy (or auto “eating” itself) in cancer cells, a critical role in the proposed mechanism of action.
They also administered submaximal doses of THC and cannabidiol together which produced a potent inhibition of growth of tumor cells (glioma xenographs). CBD is another plant-derived cannabinoid that also induces glioma cell death through a mechanism of action different from that of THC. The two work hand in glove each complimenting the others anti-cancer actions.
In their conclusion:
Moreover, treatment with TMZ and submaximal doses of THC and CBD produced a strong antitumoral action in both TMZ-sensitive and TMZ-resistant tumors. Altogether, our findings support that the combined administration of TMZ and cannabinoids could be therapeutically exploited for the management of GBM. (Mol Cancer Ther; 10(1); 90–103. ©2011 AACR.)
THC And GBM
Another Spanish trial was conducted. Entitled: A pilot clinical study of Δ9-tetrahydrocannabinol in patients with recurrent glioblastoma multiforme.[ref]British Journal of Cancer (2006) 95, 197–203.[/ref]
This time it was a pilot clinical study of THC on human test subjects with recurrent GBM. Headed by Dr Guzman they found that intracranial administration of THC directly into the tumor was safe and effective although median survival time was only 24 weeks. In conclusion:
The fair safety profile of THC, together with its possible antiproliferative action on tumour cells reported here and in other studies, may set the basis for future trials aimed at evaluating the potential antitumoral activity of cannabinoids.
There were no induced remissions in this group of only nine patients. Although this surprised me it makes some sense in terms of the entourage effect that I’ve mentioned previously. It means that in order to kill cancer cells in vivo (in real living human subjects) we might need all of the phytocannabinoids in cannabis oil.
The Entourage Effect encourages cancer cell death in vivo through synergy. In part two we’ll meet several patients who apparently beat the deadliest cancers known using the essential oil of cannabis as part of their treatment protocol.
Part Two – The Clinical Cases
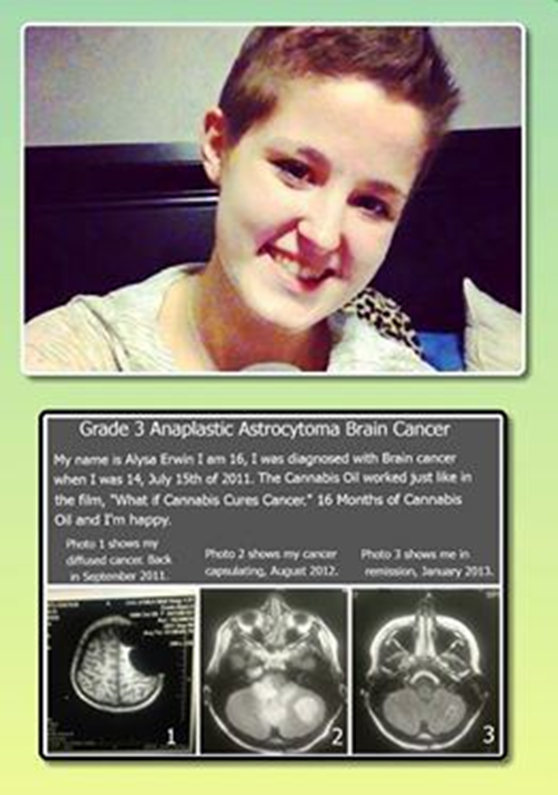 The Teen Who Beat Terminal Brain Cancer
The Teen Who Beat Terminal Brain Cancer
In part one I highlighted the carefully hidden facts that cancers are at pandemic proportions throughout the world. And for the worst cancers the cure rates have not changed in 40 years. Now let’s look at some anecdotal case reports of cannabis cures that have provided imaging studies.
At the risk of butting heads with the “evidence-based” naysayers of medical marijuana we have the case of Alysa Erwin, a fourteen year old diagnosed with terminal brain cancer in 2011. The grim diagnosis was Grade III anaplastic astrocytoma, an inoperable cancer of the brain with at best a 25% survival rate over five years. In reality her doctors told her she had two years to live, no more.
Do to the nature of the cell line the tumor spreads out like a crab with “legs” reaching deep into critical brain structures making it impossible to surgically remove. This leaves the patient with chemo or radiation as the only alternatives. They are not cures either.
DECIDED ON RSO
Prompted by her father’s research into Rick Simpson Oil (RSO), a special preparation of cannabis oil, he suggested she try it. At first she opted for conventional chemo with Temodar but after five agonizing days she was so sick it was abandoned in favor of RSO.
With the very first dose of RSO Alysa’s mood and appetite greatly improved. Over the course of the first year she increased her dose from 1.5 ml per day, quickly upping it to three milliliters per day maintenance dose.
Note: the usual cancer-killing dose of RSO is a gram per day which roughly comes out to be a cubic centimeter or milliliter. One needs to take this for at least three-four months or until the tumors are gone. The dose is usually something like taking sixty grams of RSO over ninety days.
As you can see below, the first set of images are the MRI results showing the tumor involvement in the posterior fossa (back of the head). The tumors appear as a lighter grey at the bottom portion of each image.
Below is a magnified image from a 2012 MRI clearly showing massive tumor involvement and a 2013 MRI showing her to be tumor free.

Below is the follow up MRI showing her to be in remission.
Relapse
Sadly, after 18 months of being in remission Alysa’s cancer returned in the summer of 2014. Apparently she reduced the dose of RSO as recommended but it may have been too great of a reduction. There are also reports that the family couldn’t afford RSO at some times. It suggests that there were periods of time when she was not taking anything.
What happened? It looks like there is a post-tumor phase where the RSO is still actively killing on a microscopic level long after the gross appearance of the neoplasms have vanished. How much is needed during this period? How long do patients need to continue taking RSO after the gross evidence of cancer has disappeared? Nobody knows for sure.
This is exactly why we need more carefully controlled studies.
As before she started taking full-strength RSO again. A November 2014 MRI verified the RSO was working with a decrease in tumor size. This is hugely important because it shows a re-challenge effect suggesting that the RSO is indeed an anticancer compound.
I tried to find out how Alysa was doing in 2015 but I was not able to find much useful information on her status. Her normal blogs have no 2015 entries and links no longer function. She still has a Face Book page but without anything helpful regarding her current status. I fear for the worst.
Even if she has succumbed to her cancer the simple fact that she was able to eradicate one of the most aggressive and deadly brain cancers that exists is phenomenal all by itself. This alone should prompt an intense investigation into using RSO for all children with astrocytomas period.
Case Two – Eight Month Old Baby
Below is another similar type of brain cancer cured with RSO. This time it’s an eight-month-old baby. Seen below is the MRI evidence.
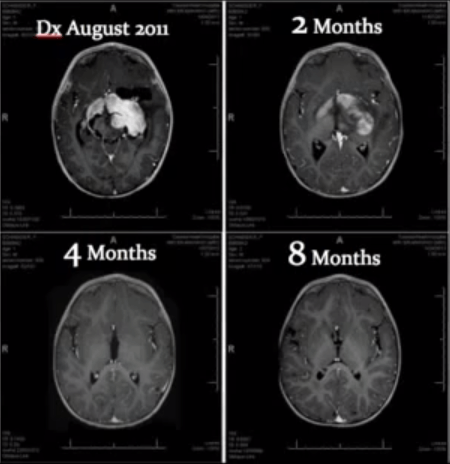
Cannabis Oil Brain Tumor Remission by Jeffrey Dach MD:
Dr. William Courtney was interviewed by the Huffington Post and talked about an 8 month old baby suffering from a malignant brain tumor (see MRI images above).
The parents declined conventional treatment with chemotherapy, and used cannabis oil (medical marijuana) instead. Miraculously, after two months of cannabis oil, the MRI scan showed dramatic improvement. “They were putting cannabinoid oil on the baby’s pacifier twice a day, increasing the dose… And within two months there was a dramatic reduction.”
The initial MRI scan at the upper left frame showed typical features of an inoperable brain tumor, with features of a “butterfly glioma” with invasion of the corpus callosum and spread across the midline, At 2 months, the follow up MRI scan shows regression of tumor, and at 4 and 8 months the scans show complete clearing, and are totally clean.
This is Highly Significant
Butterfly malignant gliomas are highly aggressive tumors, and poorly responsive to conventional chemotherapy and radiation treatment. I can tell you this type of response is never seen with conventional treatment. In my opinion this type of response is highly significant.
Dr Courtney says: “The child is a miracle baby…. we should be insisting this is frontline therapy for all children before using medications that have horrific long term side effects. (such as chemo).”[ref](http://jeffreydachmd.com/2014/04/cannabis-oil-brain-tumor-remission-jeffrey-dach-md/) 10/10/2015[/ref]
Other Related ‘Cures’ From the Use of Cannabis Oil – 23-year-old Kristina Marie
Kristina Marie diagnosed at age 23 (2013) with glioblastoma stage II. Below is her preop MRI scan showing a huge left sided (your right) brain tumor in 2013.

MRI (above) after six months of “hemp” oil. Incidentally, Kristina was also suffering from up to 20 (petite mal) seizures per day while taking the anti-seizure medication Keppra. After starting hemp oil she was able to control the seizures without medication. In the beginning she had terrible headaches, vomiting and nausea from the tumor and the medication. Eventually she was able to rid herself of all drugs while taking only hemp oil. Please note that she refers to her medication as hemp oil which is actually cannabis oil often referred to as RSO.
A recent Oct 2015 video shows that she is doing well.
Sharon Kelly
Sharon Kelly: Cannabis Killed My Terminal Stage IV non small cell lung Cancer
Above is Sharon Kelly’s image of her Jan 17 PET scan (taken from YouTube) showing the left sided five centimeter mass in her chest consistent with lung cancer.
After 7 months on RSO (started in Feb) we see the third of September image showing no tumors in the chest. This is particularly interesting because she did much of the dosing (starting in June of that year) per rectum. Dose ½ cc of RSO mixed with coconut oil which resulted in no psychoactive effects but it still shrunk her tumors very effectively. She received chemo with her treatments. The rectal route may turn out to be an alternate method of application for those who cannot tolerate the psychoactive effects.

In the above PET scan image we can see that she is entirely tumor free.
In summary I have provided cases where a tincture of marijuana seems to be a miraculous tumor-shrinking drug. This effect is seen in the most destructive and deadly cancers in existence. I highlighted astrocytomas because of their aggressiveness but I also included a case showing that stage four non-small cell lung cancer, equally as deadly, can also be safely treated using cannabis oil.
Results like these are frequently reported on YouTube and elsewhere. Based on positive results with animals GW Pharmaceuticals has plans to establish phase 1b/2a clinical trials using their proprietary Sativex which is a 1:1 mixture of THC:CBD in treating GBM. The results of this trial are pending.

Woman Rids Body of Cancer in 4 Months Using Cannabis Oil
Woman Rids Body of Cancer in 4 Months Using Cannabis Oil
Woman Rids Body of Cancer in 4 Months Using Cannabis Oil
Medical doctors and healthcare personnel alike are stymied by the miraculous cure which recently occurred to Michelle Aldrich who suffered from a deadly form of lung cancer.
Michelle was sixty-six years old at the time. Initially she developed a low-grade fever and cough which she couldn’t shake. Several months later it worsened; she developed signs of a pneumonia which prompted her to seek medical care. Her doctor ordered a CT scan trying to determine what the problem was. The scan revealed a large mass in the central region of the chest consistent with lung cancer.
NON-SMALL CELL LUNG CANCER (NSCLC)
Unfortunately the biopsy and staging of the tumor revealed it to be poorly differentiated, non-small cell lung cancer (adenocarcinoma) or NSCLC for short, stage three. All lung cancers carry a poor prognosis but this form is particularly aggressive. From the National Cancer Institute:
General Information About Non-Small Cell Lung Cancer (NSCLC)
NSCLC is any type of epithelial lung cancer other than small cell lung cancer (SCLC). The most common types of NSCLC are squamous cell carcinoma, large cell carcinoma, and adenocarcinoma, but there are several other types that occur less frequently, and all types can occur in unusual histologic variants. Although NSCLCs are associated with cigarette smoke, adenocarcinomas may be found in patients who have never smoked. As a class, NSCLCs are relatively insensitive to chemotherapy and radiation therapy compared with SCLC. Patients with resectable disease may be cured by surgery or surgery followed by chemotherapy. Local control can be achieved with radiation therapy in a large number of patients with unresectable disease, but cure is seen only in a small number of patients. Patients with locally advanced unresectable disease may achieve long-term survival with radiation therapy combined with chemotherapy. Patients with advanced metastatic disease may achieve improved survival and palliation of symptoms with chemotherapy, targeted agents, and other supportive measures.
Incidence and Mortality
Estimated new cases and deaths from lung cancer (NSCLC and SCLC combined) in the United States in 2015[ref]American Cancer Society: Cancer Facts and Figures 2015. Atlanta, Ga: American Cancer Society, 2015.[/ref]:
• New cases: 221,200.
• Deaths: 158,040.
Lung cancer is the leading cause of cancer-related mortality in the United States.[ref]American Cancer Society: Cancer Facts and Figures 2015. Atlanta, Ga: American Cancer Society, 2015.[/ref] The 5-year relative survival rate from 1995 to 2001 for patients with lung cancer was 15.7%. The 5-year relative survival rate varies markedly depending on the stage at diagnosis, from 49% to 16% to 2% for patients with local, regional, and distant-stage disease, respectively.[ref]Ries L, Eisner M, Kosary C, et al., eds.: Cancer Statistics Review, 1975-2002. Bethesda, Md: National Cancer Institute, 2005.[/ref]
Michelle was classified with having stage three or T3, involving a number of regional lymph nodes in the chest. A T4 staging means distant nodes were found to be positive for tumor metastasis. Five-year survival vastly decreases from T3 to T4.
Surgically resectable disease is generally stage I, stage II and selected stage III tumors. Generally T3 and T4 use combination modalities since surgery cannot be used solo for cure. One must also use chemotherapy and or radiation.
But let’s face it, survival for this type of cancer hasn’t improved since the war on cancer began in the seventies as Dr Abramson reminds us. In his pivotal book “Overdosed America,” he explains that the age-adjusted death rate for all cancers has actually increased since the “war” began. Put simply: you are no better off today with most cancers than you were 45 years ago. Unless you have the courage to venture outside the conventional medical “box.”
ASTONISHING CURE IN LESS THAN FOUR MONTHS
At best using conventional medicine Michelle had an approximately 49% five year survival and that’s with only local tumor involvement. It drops quickly as you can see from above down to 2% five year survival with distant stage disease.
“I thought I was going to die,” Aldrich says from her Marina District apartment. But she didn’t. And now, she is busy telling anyone who will listen that, along with diet and chemotherapy, a concoction of highly concentrated cannabis oil eliminated her cancer in less than four months.[ref](http://www.sfweekly.com/sanfrancisco/miracle-cannabis-oil-may-treat-cancer-but-money-and-the-law-stand-in-the-way-of-finding-out/Content?oid=2825695) 09/22/2015[/ref]
Initially diagnosed in January of 2012 and by April 2013 a repeat CT scan showed a reduction in tumor size by 50%. What tumor remained was surgically removed. Repeat CT scan showed no tumor involvement anywhere in the chest.
Her doctors — one of whom noted the effect of “homeopathic treatments, including hemp oil” to reprogram the cancer cells to kill themselves — “are floored,” she says. “They’ve never seen anything like it.”[ref]IBID[/ref]
CONFUSED?
See how confusing the nomenclature is? To clarify, Michelle did not use “hemp oil” she used cannabis oil which is completely different. Specifically she used Rick Simpson Oil (RSO), AKA Phoenix Tears. It is also not homeopathic in any sense of the word. RSO is allopathic all the way; it acts much like a powerful drug, as powerful as any pharmaceutical. In fact, it appears to be much more effective than any chemotherapeutic currently on the formulary.
Using “hemp oil” which is the essential oil extracted from industrial hemp, to treat ANY disease is a fool’s errand. Only authentic cannabis oil can cure cancers. Please be aware of that fact. Industrial hemp is good for food-grade seeds, its bright green oil can be used in salads. It’s also good for textiles and paper but when you want to cure disease you need the big guns that real cannabis employs.
MEET CONSTANCE FINLEY
In the East Bay area of San Francisco where I had my medical practice lives a woman who is very well known to the cancer community. She is a very busy person. While the webpages of the NCI claim that there is no evidence that cannabis cures cancers, we have plenty of real-time and anecdotal case reports of numerous cures of “incurable” late stage, highly aggressive tumors. Some of those reports come from Constance Finley.
Employing the same manufacturing techniques seen on Rick Simpson’s website, she takes a pound of cannabis and reduces it into one ounce of pure medical magic.
This cannabis reduction sauce (essential oil) in its thickened final stage is called Rick Simpson Oil (RSO).
Most oncologists would guffaw over the idea that the sap of a common weed could defy the realm of possibility and outperform the best that Big Pharma can deliver. But it can and it does. The internet is overflowing with anecdotal cures of virtually any cancer regardless of cell type. Doctors and laypersons alike would never believe it was possible were it were not for the scores of bona fide, documented, cases seen by this woman and many others.
She was quoted as saying that there is a world-class oncologist in San Francisco who has already referred 26 “deaths door” patients to her in 2013. All 26 of Finley’s referrals had stage 4 cancers. The patient population included brain tumors, colon cancers, and lung cancers to name a few. Stage four is a death sentence since it means the malignant cells had escaped the primary tumor and metastasized to other organs. Most had only a few months to live, some had less than six weeks. All patients received modern medical treatments such as chemotherapy with the concentrated oil. She reportedly has “cured” all but one of them. That’s a 96% cure rate, the best in the business if it’s true. And it’s not just in San Francisco.
These survival stories are becoming more common. One of the most high-profile was the case of Montana toddler Cash Hyde, diagnosed with a brain tumor at 20 months, whose family credits cannabis oil for keeping the tumor at bay and keeping him alive — until a change in Montana state law cut off his access to oil for a few months. The tumor returned and he died in November, at age four.[ref](http://www.sfweekly.com/sanfrancisco/miracle-cannabis-oil-may-treat-cancer-but-money-and-the-law-stand-in-the-way-of-finding-out/Content?oid=2825695) 09/24/2015[/ref]
A LOW PROFILE
Understandably this San Francisco oncologist prefers to keep his name private when being quoted. Even when a powerful remedy like this mops up cancer cells like a Pickwickian tween in a pie-eating contest, academics still prefer to remain hidden lest they succumb to the predictable harassment and ridicule of their peers. Some could easily lose their jobs should they become overzealous reporting the truth that a simple plant extract outperforms the best chemo by an unbelievably wide margin.
One question. When will these oncologists start referring patients to Finley before the system nearly kills them? Imagine how helpful it could be then.
WIDE SAFETY MARGIN
Remember also that RSO is NON-TOXIC. There is no devastating blowback from using it. Contrast this to your typical chemotherapy course which causes blood cancers years later in up to 15% of patients who received chemo at some point earlier in their disease course. Furthermore, chemotherapy is an efficient immune system destroyer. Just what you don’t need when fighting for your life.
Meanwhile, by definition late stage cancer is incurable and always leads to 100% mortality. This makes RSO even more astonishing. That’s because these people are written off by modern medicine as failures where nothing could help them. Sick, emaciated from chemo and radiation, cachectic and nearly dead she revives them like a modern day Lazarus factory.
Take a moment to reflect on this humble fact. It reveals to us the absolute beauty of this incredible, health-regenerating, symphony of phytocannabinoids. A true gift from God.
If it’s all true. And that’s a big if. We need controlled studies now more than ever before. But don’t hold your breath. Clinical trials are ten years away, minimum.
EASY AS BOILING WATER
To make this unpretentious oil is actually very easy. Simply go to Rick Simpson’s website for instructions. The most important of all is that you use a safe solvent for extraction. Aldrich’s providers use Everclear in making what they call “Milagro oil” which is the same as RSO, at Wo/Men’s Alliance for Medical Marijuana in Santa Cruz, CA. Finley’s operation uses isopropyl alcohol which can be toxic in large doses. Theoretically you will boil off all of the isopropyl alcohol but personally I think it’s far better to use ethanol the only truly safe alcohol (in small doses).
Once they have procured the precious oil patients with end-stage disease need to ramp up to an anti-cancer blood level as soon as humanly possible. But the material is extremely potent: a concentrated extract clocking in at around 70% active THC or higher. The oil is a reduction using heat so all of the acidic cannabinoids are converted to psychoactive decarboxylated forms of which THC is a major component.
THE ENTOURAGE EFFECT
But it’s not just the THC that they need. All of the 60 phytocannabinoids, decarboxylated and ingested along with the terpenes, and thousands of other mysterious chemicals found in the oil, produce the “entourage effect.” Scientists have speculated that this synergy is the real reason why RSO is so strangely effective. You need whole plant extracts of real cannabis to knock cancer cells into next week. The potent psychoactivity is the biggest hurdle to overcome.
That’s why patients need to start out with a dose that will not pound them into submission the first day which may discourage its use. Practitioners who use the drug regularly recommend starting out with a small rice grain sample of the sticky oil, rub it inside your mouth along the gum line. After that you simply swallow it. From there you quickly work your way up to dosing four times a day or more. For those familiar with the high of cannabis they can accelerate the dosing very quickly if they like the way they feel. You’ll be doing a lot of sleeping since the preparation normally comes from an indica only species. No sativas are used since the preparation becomes too speedy for most patients especially at high dosages. Sleep induces healing. It’s all part of the process: eat, sleep, relax, protect, and don’t forget…forget.
With perseverance one can increase the dose rapidly to full-strength in one week. You’ll want to increase the dosing of a “rice grain” to four time a day or more to achieve a total of one gram per day. So each dose is about ¼ gram. At that point blood levels are high, we start to see the magical entourage effect take place. Tumors shrink and finally disappear to be replaced with healthy cells.
HOW MUCH?
The cost? At a gram per day one needs to take it until the cancer is gone which is at least four months. A pound of quality (organic) Indica which is what they prefer to use to help you sleep and heal, runs about $2,500 to $3,000 in the Bay Area. Aldrich says a three-month regimen costs her $1,200 a month; Finley charges $5,500 for a two-month cycle.[ref]IBID[/ref] That’s pricey but compared to what?
A typical cancer patient caught in the Commercial Sick Care System (CSCS) could buy a (used) Bentley with the money they need for chemotherapy and radiation. In the US they will on average spend eighty thousand dollars toward chemotherapeutics during the last two years of life and often die in spite of “cutting edge” therapy. When viewed this way cannabis oil looks exceedingly cheap and very worthwhile. With the added bonus-you get to live.
The statistics tell us either you pay eighty thousand over two years for the right to die in pain, anguish, and loss of dignity; or you shell out eleven thousand on RSO and possibly receive a new lease on life. I don’t know that’s a tough choice.
Furthermore, patients with NSCLC who have survived their ordeal often develop secondary lung cancers years later as a matter of course.
Not so with RSO. Taking a lower maintenance dose of RSO after the tumors disappear is highly recommended since it will help prevent the ignoble recurrence of tumors.